Peroneus quartus muscle.



Clinical History
The patient (a woman of 28 years of age) was referred to our department as an outpatient for MRI of her right ankle with the indication of unspecific lateral ankle pain.
Imaging Findings
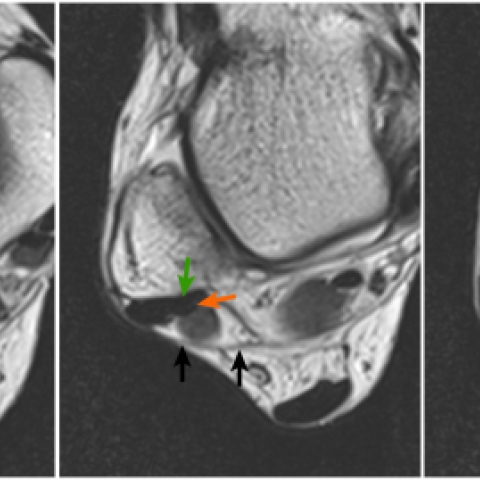
The MR examination included T1W, T2W, T2W/TSE with fat suppression and STIR sequences in three planes. The muscle belly of the soleus muscle was extending lower than usual [fig.1, 2]. There was a small amount of fluid in the tibiotalar joint mainly laterally at the level of the lateral malleolus [fig.2]. Behind the peroneal tendons, beneath the superior peroneal retinaculum, an additional mass was revealed. The signal intensity of this mass equalled that of muscle on all pulse sequences [fig.1, 2]. A linear low signal intensity structure, resembling a tendon, was also seen within the aforementioned mass. This low signal structure was inserting into the peroneus brevis tendon just caudally to the fibular tip [fig.1, 2, 3]. The findings were interpreted as a peroneus quartus muscle because of its location and tendon insertion.
Discussion
The lateral compartment of the leg includes: The peroneus longus muscle which arises from the proximal fibula and the peroneus brevis muscle which arises from the lower two-thirds of the fibula [1]. They contribute the peroneus longus tendon (PLT) and the peroneus brevis tendon (PBT) respectively [1]. At the level of lateral malleolus the PBT lies anteriorly, in the peroneal groove of the distal fibula [1]. The superior peroneal retinaculum encircles both tendons at the level of the lateral malleolus [1]. PLT inserts onto the base of the 1st metatarsal and 1st cuneiform, and PBT onto the tuberosity of the 5th metatarsal [1]. In our case MRI identified both muscles and tendons.
In 83%–95% of cases a third peroneal muscle is found, the peroneus tertius [2], which lies in the anterior compartment of the leg. Its tendon passes through the inferior extensor retinaculum and inserts onto the base and the dorsal surface of the shaft of the 5th metatarsal [2]. In our case MRI did not disclose this muscle.
Besides these muscles, there are numerous accessory muscles at the distal lateral aspect of the leg. They include peroneus quartus, peroneus accessorius, peroneocalcaneus externum, and peroneus digiti minimi muscles [3]. It was suggested that they all should be referred with the term peroneus quartus muscle (PQM) [3]. They have a prevalence ranging from 10% (MRI studies) [4], to 26% (cadaveric studies) [3]. In our case MRI disclosed a muscle belly, lying behind PBT and PLT. This finding could represent a low situated belly of the peroneus brevis muscle, but a separate tendon within this muscle tissue was recognized. This tendon was inserting into the PBT just caudally to the fibular tip, so it represented a PQM.
It is difficult for the clinical examination to define the exact cause of unspecific lateral ankle pain, so MRI is needed. The PQM may be responsible for unspecific pain in the lateral aspect of the ankle [5], as in our case. It may also provoke a feeling of fullness at the level of the lateral malleolus, or it may be found incidentally [5]. The patient in our case was treated conservatively and the pain subsided within three weeks.
Differential Diagnosis List
Final Diagnosis
Peroneus quartus muscle.
Liscense
Figures
T1W/TSE/AXIAL

T2W/TSE/AXIAL
T1W/TSE/CORONAL

Medical Imaging Analysis Report
I. Imaging Findings
1. MRI shows that the lateral tendons and muscle structures of the right ankle joint are clearly visible. The peroneus longus tendon (PLT) and the peroneus brevis tendon (PBT) can be identified, both running within the fibular groove of the lateral malleolus.
2. A supplementary muscle belly image can be observed posterior to both PBT and PLT. Near the PBT, a separate tendon structure can be seen, inserting into the PBT tendon tissue near the distal fibula, consistent in shape with the peroneus quartus muscle (PQM).
3. No obvious tenosynovial effusion, tendon rupture, or significant bony destruction is observed around the lateral malleolus. The articular surfaces and ligaments appear relatively intact as a whole, with no significant traumatic changes.
II. Possible Diagnoses
Based on the above imaging findings and the patient's clinical symptoms (unexplained lateral right ankle pain), the possible diagnoses include:
- Peroneus Quartus Muscle (PQM) with lateral ankle discomfort: A variation in the peroneal muscles can cause crowding or friction in the lateral malleolus area, leading to nonspecific pain.
- Peroneal Tendinitis/Tenosynovitis: Overuse or prolonged friction of the lateral tendons can also result in chronic pain.
- Mild lateral ankle ligament injury: Although no obvious tear or laxity is seen on imaging, mild ligament-related discomfort may still be present.
III. Final Diagnosis
Taking into account the patient’s age (28 years), symptoms (persistent pain in the lateral ankle), physical examination findings (no clear evidence of significant ankle ligament damage), and MRI showing a marked variation of the peroneal muscle group (an additional tendon is visible), the most likely diagnosis is:
Lateral ankle discomfort caused by the Peroneus Quartus Muscle (PQM).
Because this anomalous muscle can create a sense of fullness in the lateral malleolus region or cause friction with surrounding tendons, it may induce pain. Combined with the imaging features and clinical symptoms in this case, the above diagnosis can be established.
IV. Treatment and Rehabilitation Plan
- Rest and avoidance of activities that exacerbate symptoms: During the acute phase or when pain is significant, reduce running, jumping, and weight-bearing activities.
- NSAIDs or appropriate analgesics: Short-term use during pain episodes can help relieve pain and inflammation.
- Local physical therapy: Such as ultrasound, alternating cold and hot compresses, or low-frequency electrical stimulation to promote local blood circulation and reduce pain.
Early Stage (Pain Relief Phase, approximately 1-2 weeks):
- Isometric exercises for the ankle: Perform light, pain-free resisted movements of the ankle, such as isometric dorsiflexion, plantar flexion, eversion, and inversion.
- Range of motion exercises: Passive or active movements of the ankle within a pain-free range to enhance soft tissue elasticity.
Intermediate Stage (Pain Gradually Subsiding, approximately 2-4 weeks):
- Elastic resistance band exercises: Gradually increase the load by performing resisted ankle eversion, plantar flexion, and dorsiflexion, strengthening the peroneal muscles and lower leg muscle power.
- Balance training: Use a balance pad or single-leg stance to improve ankle proprioception and stability.
Late Stage (Pain Almost Gone, approximately 4 weeks and onward):
- Progressive weight-bearing exercises: Gradually increase difficulty and volume in running, jumping, and directional changes, simulating daily or sports scenarios.
- Functional exercises: Combine lower limb core training and full-body coordination (e.g., balance board, crossover steps) to enhance dynamic control of the ankle.
If conservative treatment is ineffective and the patient continues to experience significant lateral ankle pain or functional limitations, surgical removal or repair of the anomalous tendon may be considered. However, this is rarely performed and requires careful evaluation.
- Frequency: 3-4 times per week, adjusted according to pain response.
- Intensity: Start at approximately 25%-30% of perceived exertion, gradually increasing to a moderate intensity.
- Time: 20-30 minutes per session, including 20% warm-up, 60% main training, and 20% stretching/cool-down.
- Type: Focus on ankle stability and muscle strengthening exercises, combined with full-body coordination training.
- Progression: Increase exercise load or difficulty every 1-2 weeks based on pain and fatigue levels.
Disclaimer
This report is based on current imaging data and clinical history for reference only and cannot replace an in-person consultation or professional physician’s face-to-face evaluation and diagnosis. If there are any further changes in symptoms or questions, it is recommended to seek medical advice promptly and undergo related examinations or treatments.
Human Doctor Final Diagnosis
Peroneus quartus muscle.