Tropical Pyo-myositis and septic arthritis



Clinical History
A 16-year-old male patient presented with a diffuse painful swelling of the left thigh and right forearm, fever (39 °C) and limping. His total blood count revealed leukocytosis with absolute neutrophilia. The patient had negative laboratory results for HIV, hepatitis B and C viruses, diabetes mellitus and Still’s disease.
Imaging Findings
With ultrasound of the left thigh an intramuscular abscess was noted in the vastus intermedius. Ultrasound of the right forearm showed another abscess. Aspiration produced pus. Culture of the aspirate revealed methicillin sensitive staphylococcus aureus pathogen.
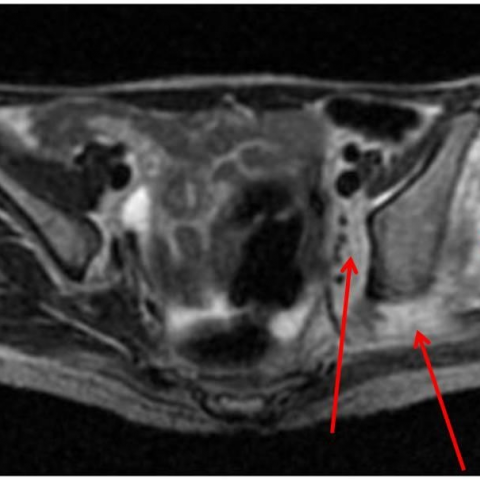
Left hip MRI revealed oedema in the muscles surrounding the left hip joint. The abscess was only a small component in the proximal vastus intermedius muscle. The left hip joint revealed synovial thickening, marked joint effusion with subluxation of the femoral head and bone marrow oedema in the acetabulum, femoral epiphysis, neck, trochanters and upper shaft. Cortical interruption was seen in the acetabulum and femoral head revealed deformity of its contour.
MRI of the right forearm showed an abscess on the antero-lateral aspect. It was surrounded by extensive oedema in all forearm muscles and bone marrow oedema of the radius and ulna, with no intra-articular extension. Another separate abscess was seen in the antecubital fossa.
Discussion
Tropical myositis (pyomyositis) is a disease of tropical and developing countries. It is an acute muscular infection that is usually caused by bacterial pathogens, commonly staphylococcus aureus. The infection is the result of hematogenous spread.[1, 2] It is believed to originate from transient sub-clinical bacteremia from an occult focus.
The disease is now recognized in immune compromised subjects, e.g. AIDS, diabetes mellitus and transplant patients.[1-4]
A single muscle group affection is the common form; multiplicity is recorded in 10-20%.[1]
The disease is common in children and adolescents with slight male predominance. It has 3 stages. First stage starts with subacute onset of variable fever, pain, swelling with minimal systemic manifestations. This stage may divert the clinician to more common diseases, e.g. osteomyelitis. The second (Suppurative) stage is characterized by high grade fever and systemic symptoms. Because of the deep seated location and the tense overlying muscles, the classical signs of abscess formation, e.g. fluctuation may be lacking. The third stage occurs if proper treatment is not initiated, e.g. dissemination of infection, septic shock and acute renal failure.[5]
Imaging is essential for patient management. The abscess is the hallmark of pyomyositis.
On ultrasound, the abscess appears as a cystic lesion within the muscle, with internal echoes and trabeculations. Ultrasound is available, safe, and cheap. But it has poor sensitivity for detection of early stage and the deep extension of the abscess is difficult to assess, especially in obese patients.[6]
On CT, an abscess appears as a well defined low attenuation lesion with thin peripheral enhancement after IV contrast injection. Contrast enhanced CT may help detect the extension of infection.
MRI is preferred as the diagnostic tool of choice. An abscess appears as a cystic lesion that is hyperintense on T2W and STIR with thin peripheral enhancement after IV injection of gadolinium. The surrounding muscles and bones show diffuse oedema. MRI is not always available, not to mention, that it requires sedation in young children.
Diagnosis is confirmed by the aspiration of pus from these abscesses.
It is still unknown whether joint involvement is the cause or complication of pyomyositis.[7] Because pyomyositis is common in children and in the thigh, the differentiation between septic arthritis and pyomyositis is important. Clinically, this is impossible.
MRI has the potential to improve the clinical outcome by giving a more precise anatomical diagnosis to differentiate tropical pyomyositis from other more common diseases in the same age group, like osteomyelitis and septic arthritis.
Differential Diagnosis List
Final Diagnosis
Pyomyositis (Tropical myositis) with complicated left hip septic arthritis.
Liscense
Figures
Ultrasound


Left thigh MRI



Right forearm MRI



Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided ultrasound and MRI images, the following key features are observed:
- Abnormal fluid collections are noted in the muscle tissues of the left thigh and right forearm, containing small echoes or heterogeneous signals, suggesting pus or exudate, consistent with a muscle abscess (purulent collection).
- Ultrasound demonstrates relatively well-defined lesions appearing as “cystic” hypoechoic areas with uneven internal echoes, possibly with septation or flocculent echoes.
- On MRI, T2 and STIR sequences reveal hyperintense signals within the lesions. Post-contrast images show ring or thin-layer enhancement with surrounding muscle signal changes indicative of inflammatory edema or infection.
- The lesions are relatively deep, with significant local soft tissue swelling, possibly involving diffuse edema in the surrounding muscle.
II. Potential Diagnoses
Given the patient’s age (16-year-old male), fever, local pain, and swelling, along with imaging findings suggestive of intramuscular purulent collections, the following differential diagnoses should be considered:
- Tropical Pyomyositis (Purulent Myositis)
- Commonly caused by Staphylococcus aureus via hematogenous spread, leading to infection within the muscle and abscess formation.
- Frequently seen in adolescents. Clinically presents with high fever, pain, and swelling, and imaging typically shows intramuscular abscesses.
- Osteomyelitis or Related Complications
- Infection involving adjacent bone structures may affect nearby soft tissues. Although primarily involving bone, this possibility should be ruled out. MRI can help clarify any bony involvement.
- Septic Arthritis
- If a joint space is infected, nearby soft tissues can show inflammatory changes or abscess formation. However, in this case, the main findings are intramuscular collections, and joint involvement is not prominently indicated.
- Other Soft Tissue Abscesses or Inflammatory Lesions
- For example, cellulitis, but this typically presents as more diffuse superficial infection rather than a singular or multiple deep abscesses.
III. Final Diagnosis
Based on the patient’s age, clinical presentation (fever, pain, limping, elevated white blood cell count), and ultrasound/MRI evidence of multiple intramuscular abscesses, the most likely diagnosis is:
Tropical Pyomyositis (Purulent Myositis).
For confirmation, clinical practice typically involves abscess aspiration or surgical drainage to obtain pus for bacterial culture. When considering differential diagnoses (e.g., osteomyelitis, septic arthritis), MRI details or further imaging and laboratory tests (such as pathogen culture) are crucial for definitive differentiation.
IV. Treatment and Rehabilitation Plan
Given the diagnosis of tropical pyomyositis, the recommended treatment plan mainly includes:
-
Antimicrobial Therapy
- Empirical antibiotics targeting Staphylococcus aureus, such as cephalosporins or anti-staphylococcal penicillins, adjusted according to local pathogen profiles or sensitivity results.
- The treatment duration is typically lengthy, usually at least 2-4 weeks, with adjustments based on clinical and inflammatory marker trends.
-
Abscess Drainage
- For larger fluid collections, ultrasound or CT-guided aspiration/drainage or surgical drainage can be performed to remove pus and clear the infectious focus thoroughly.
-
Symptomatic Supportive Care
- Use of analgesics, antipyretics, and other supportive measures as needed to maintain fluid and electrolyte balance.
-
Rehabilitation and Exercise Prescription
- During the acute phase, rest and immobilization are recommended to avoid excessive weight-bearing. Once inflammation and pain subside, progressive functional exercises can be introduced.
- Early-stage rehabilitation may start with low-intensity passive range-of-motion exercises or isometric muscle contractions to improve blood circulation and reduce muscle atrophy.
- When swelling and pain have significantly improved, exercise intensity can be gradually increased based on the “FITT-VP” principle (Frequency, Intensity, Time, Type, Volume, Progression):
- Frequency: 3-4 sessions per week, adjusted to individual tolerance.
- Intensity: Start with light to moderate perceived exertion, avoiding severe pain.
- Time: Begin with 10-20 minutes per session, gradually increasing to 30 minutes or more.
- Type: Range-of-motion exercises, light resistance training (e.g., resistance bands, low-weight equipment), or low-impact aerobic activities such as cycling or swimming.
- Progression: Modify the intensity or duration approximately every 1-2 weeks according to pain and fatigue levels.
- Volume: Gradually increase weekly exercise volume, closely monitoring muscle response to prevent overtraining.
- If there is coexisting bone fragility or other systemic conditions, avoid high-load movements and ensure close monitoring during rehabilitation.
Disclaimer: The above report provides a reference-based medical analysis and does not replace an in-person consultation or professional medical advice. Patients should receive personalized diagnosis and treatment plans under the guidance of a qualified medical professional.
Human Doctor Final Diagnosis
Pyomyositis (Tropical myositis) with complicated left hip septic arthritis.