


Patient presented with 3-weeks history of anterior right knee pain following direct fall onto his knee while playing football. On physical examination, there was tenderness at the patellofemoral joint. The patella tracked normally with no joint instability. The patient was treated with immobilization for approximately 3 weeks and anti-inflammatory agents.
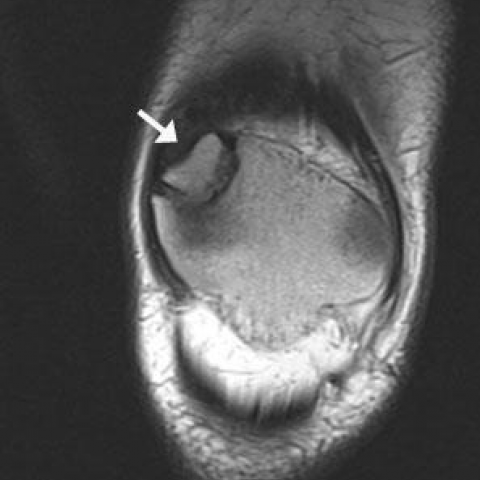
The anteroposterior radiograph of the right knee showed a wide radiolucent line coursing across the superolateral margin of the patella, with smooth, well-corticated opposing margins (Fig. 1). Magnetic resonance imaging was performed for assessment of associated internal derangement or occult injury. Proton-density (PD) MR images revealed division of the patella in two parts (Fig. 2). On the fat-saturated PD images, there was minimal bone marrow oedema (Fig. 3). Gradient echo MR images showed smooth, hyaline cartilage covering the articular surfaces on both sides of the divided patella, proving the presence of synchondrosis between them (Fig. 4). Indeed, the signal characteristics of the cartilage between the patella and the ossicle were similar to those of articular cartilage. Inversion recovery MR images showed minimal fluid within the patellofemoral joint (Fig. 5).
Bipartite or multipartite patella is a normal anatomic variant found in 2-6% of the population. Morphologic variation results from developmental union failure of one or more accessory ossification centers [1, 2]. Bipartite patella is bilateral in 30-40% of patients, and is more common in men than women, with a ratio as high as 9:1 [3-5]. Definitive diagnosis of bipartite patella can be made around 12 years of age when the accessory ossification centers normally coalesce [2, 3].
The pathogenesis of bipartite patella has not been elucidated. It has been suggested that the biomechanical pull of the vastus lateralis and the relatively poor blood supply of the superolateral patella may cause growth inhibition of the secondary ossification center leading to a synchondrosis rather than bony union [6-8]. Bipartite patellas are classified into 3 types. Type I is located at the inferior pole (5% of all cases), type II is at the lateral patellar border (20%), and type III is at the superolateral margin (75%). Our case had bipartite patella, type III.
Bipartite patella is usually an asymptomatic variant. Only 2% of patients have symptoms including patellar tenderness on palpation, or pain with knee extension. Pain onset is gradual and often after repetitive strenuous exercise, which is probably caused by overuse and imposed microtrauma to the synchondrosis. Acute pain is rare caused by fracture or disruption of the synchondrosis [9, 10]. Our case was challenging as the patient had also sustained acute direct trauma to the knee while falling onto his patella. Although the margins between the two osseous components of the synchondrosis are usually smooth, occasionally in younger patients, margins may be irregular and this irregularity might be mistaken for fracture [6].
On MR imaging, the articular surfaces of each ossicle are invested by normal hyaline cartilage, with T1-weighted and PD intermediate-, and T2-weighted intermediate-to-high signal intensity. Less commonly, fibrous tissue of hypointense signal on T1- and T2-weighted sequences may be seen [5]. In symptomatic patients with bipartite patella, bone marrow edema between the ossicles, evident as high signal intensity on T2-weighted images with fat saturation and low signal on T1-weighted images may suggest abnormal motion with disruption of synchondrosis. The synchondrosis may also contain fluid of high signal intensity on T2-weighted and inversion recovery MR images [5].
Our patient was not aware of the presence of bipartite patella. Three weeks later incidental discovery of this anatomic variant he was ambulatory again.
Bipartite patella




Based on the provided X-ray and MRI images, there is a relatively regular, smooth-contoured extra bony mass at the superolateral margin of the right patella, connected to the main patella by what appears to be cartilaginous or thin fibrous tissue. On MRI, the corresponding site shows intact cartilage signal with mild local edema, but no obvious fracture line is seen. No significant abnormalities are noted in other intra-articular structures, including the femoral condyles, tibial plateau, and surrounding soft tissues. No remarkable pathological changes are found in the remaining patellar articular surfaces. Overall, the male patient’s knee joint structure appears largely intact, with no obvious ligament or meniscal damage.
This type of abnormal bony fragment is commonly located at the superolateral margin of the patella (approximately 75% of all cases). It is typically connected to the main patella by cartilage or fibrous tissue and results from incomplete bony fusion of secondary ossification centers during development. Clinical symptoms are often minimal, but repeated stress or acute trauma can lead to local pain or swelling.
Direct trauma to the patella raises suspicion of a fracture. However, fractures usually present with sharp fracture lines, irregular fragment edges, and are often accompanied by soft tissue swelling and significant local pain. In this case, imaging shows relatively smooth and well-aligned margins in the bony region, and MRI does not indicate a definite fracture line or displacement. Thus, the likelihood of fracture is low.
Post-traumatic or repeated impact can lead to patellar bone bruising, clinically manifested as anterior knee pain. On imaging, this typically appears as localized bone marrow edema or cartilage surface damage. In this case, other than mild edema, the overall joint cartilage appears intact with no clear sign of cartilage tearing.
Combining the patient’s age, history of trauma, clinical presentation, and imaging findings, the most likely diagnosis is:
“Congenital bipartite patella (superolateral type, Type III) accompanied by mild patellar contusion.”
Although the patient has experienced knee trauma, the imaging does not show typical acute fractures or significant soft tissue damage. Therefore, a congenital variant is primarily considered, with the trauma causing local irritation and pain. If there is still concern, follow-up imaging can be performed to monitor any changes in local bone and cartilage.
Conservative Treatment:
Rehabilitation/Exercise Prescription (FITT-VP Principle):
Disclaimer:
This report is a reference analysis based on the available imaging and clinical information and should not be considered a definitive basis for diagnosis or treatment. Actual diagnosis and treatment should be made in conjunction with in-person consultation and expert medical advice.
Bipartite patella