Solitary plasmacytoma involving C5 and C6 vertebrae with \'Mini brain\'appearance



Clinical History
55-years-old male patient presented with quadriparesis and neck pain after trivial trauma.
Imaging Findings
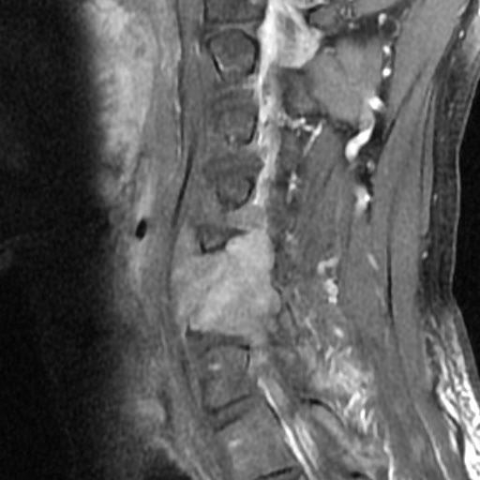
MRI cervical spine revealed altered signal intensity lesion involving vertebral body, right articular process, right transverse process, right pedicle of C5 and C6 vertebra, right lamina of C6 vertebra and right-sided facet joint between C5 and C6 vertebrae.
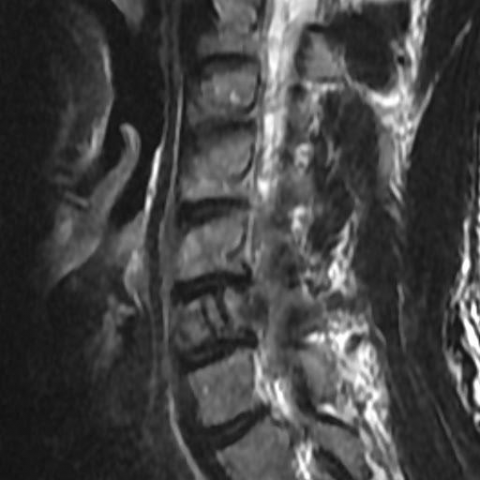
The lesion appeared hyperintense on T2/STIR sequences and hypointense on T1 sequence. The lesion showed intense homogeneous enhancement on post-contrast study.
The lesion extended into the right-sided prevertebral and paravertebral region at C5 and C6 vertebral level. The lesion was encasing the right vertebral artery, extending into the epidural region on the right side and causing compression and left side displacement of the cervical spinal cord at C5 and C6 vertebral level.
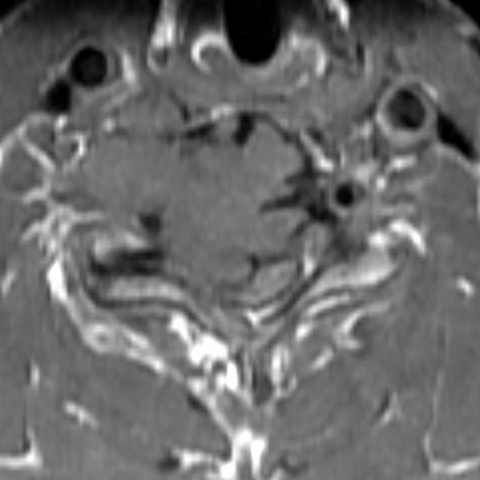
There were thick cortical struts in the C6 vertebral body predominantly on the left side. These struts were hypointense on T2/T1 images and the surrounding lesion hyperintense on T2 images. These struts resembled sulci of brain and the lesion looked like gyri of brain, showing a "Mini brain” sign in the axial images.
Discussion
A plasmacytoma is a discrete, solitary mass of neoplastic monoclonal plasma cells in either bone or soft tissue (extramedullary). It can be considered as a singular counterpart of multiple myeloma. [1]
Solitary plasmacytomas can be divided into two groups according to location: plasmacytoma of the skeletal system / solitary bone plasmacytoma and extramedullary plasmacytoma. [2]
A solitary bone plasmacytoma may involve any bone, but it has a predisposition for the red marrow-containing axial skeleton, mainly spine, rib, sternum, clavicle, skull or scapula. [2, 3]
Diagnostic criteria for solitary bone plasmacytoma are: single area of destruction due to clonal plasma cells, bone marrow plasma cell infiltration <5% of all nucleated cells, absence of osteolytic bone lesions or other tissue involvement, absence of anaemia, hypercalcaemia or renal impairment, low or absent serum / urine monoclonal protein, preserved levels of uninvolved immunoglobulins. [4]
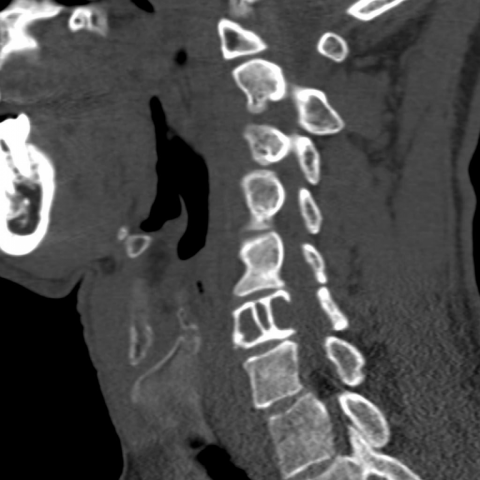
X-ray and CT show expansile lytic lesions. MRI shows expansile soft tissue intensity lesions, which appear hyperintense on T2 / STIR and hypointense on T1 images. On post-contrast study, plasmacytoma shows variable moderate to intense enhancement. [3]
In solitary vertebral body plasmacytoma, thick cortical struts form in the vertebral body. The characteristic appearance of thickened cortical struts is probably a result of a stress phenomenon from the lytic process of the plasmacytoma forcing the remainder of the bone to increase thickness as a compensatory response to weakening bone. Perhaps an explanation of this appearance, which is not seen in other primary bone or metastatic spine lesions, concerns the less aggressive nature of plasmacytoma compared with other tumours that destroy bone. The cortical thickening in the arrangement of plasmacytoma appears to be unique in this tumour. This appearance can also be seen on CT of plasmacytoma. [3]
In our case, biopsy was performed and plasmacytoma could be confirmed.
Teaching point: A “mini brain” appearance in an expansile lesion of the vertebral body is pathognomonic of solitary plasmacytoma. It is important to appreciate this finding because it may help radiologists recommend appropriate laboratory studies and facilitate early and appropriate treatment. For the patient, an early diagnosis on MR imaging may obviate biopsy. [3]
Differential Diagnosis List
Final Diagnosis
Solitary plasmacytoma involving C5 and C6 vertebrae with "Mini brain"appearance
Liscense
Figures
MRI cervical spine - post-contrast sagittal T1 fat sat images



MRI cervical spine - post-contrast coronal T1 fat sat images


MRI cervical spine - post-contrast axial T1 fat sat images




MRI cervical spine - sagittal T2 images



MRI cervical spine - axial T2 GRE images




MRI cervical spine- axial T1 images

CT cervical spine - sagittal reformatted images

CT cervical spine - axial reformatted images

CT cervical spine -coronal reformated images

1. Imaging Findings
Based on the MRI and CT images of the cervical spine provided by the patient, a noticeable expansive lesion can be observed in the cervical vertebral body, exhibiting a “mini-brain” appearance on imaging. The specific features are as follows:
- Lesion Location and Morphology: The lesion is located in the cervical vertebral body (primarily involving certain segments of the cervical spine, as deduced from the images), presenting with expansion, bone destruction, and irregular local structural changes.
- Density/Signal Changes:
- CT Findings: An enlarged lytic lesion is seen, with localized thickening of the vertebral cortical bone maintaining some of its shape, forming a “thick bony trabeculae” structure.
- MRI Findings: On T1-weighted images, the lesion appears hypointense; on T2/STIR-weighted images, it appears hyperintense, with moderate to marked enhancement observed inside and around the lesion.
- Involvement of Surrounding Tissues: The lesion leads to weakened local vertebral structure, with compression or invasion of the adjacent spinal canal, resulting in varying degrees of spinal cord compression. A mass-like change can also be seen in the soft tissue.
2. Potential Diagnoses
Considering the patient’s age, symptoms (neck pain and quadriparesis triggered by minor trauma), and imaging findings, the following differential diagnoses can be taken into account:
- Lytic Metastasis: Most metastatic tumors can present lytic changes and typically progress quickly. The “thick cortical trabeculae” or “mini-brain” appearance is not commonly noted.
- Multiple Myeloma/Solitary Plasmacytoma (Osseous Plasmacytoma): Typical manifestations include expansive lytic lesions with well-defined margins, usually low signal intensity on T1-weighted images, and associated soft tissue masses. The distinct “mini-brain” appearance is characteristic of solitary plasmacytoma, caused by thickened trabeculae in the vertebral body.
- Other Primary Bone Tumors (e.g., Chordoma, Giant Cell Tumor): They may also show expansive changes with lytic destruction, but their common locations and imaging features differ from osseous plasmacytoma (e.g., chordoma often occurs in the clivus or sacrum; giant cell tumors typically occur at epiphyseal regions of long bones). Their signal characteristics vary as well.
- Infectious Lesions (e.g., Osteomyelitis, Spinal Tuberculosis): These can cause bone destruction and soft tissue masses but generally involve the paravertebral region or intervertebral discs, showing prominent inflammatory signs and elevated clinical infection markers.
3. Final Diagnosis
Combining clinical information (a middle-aged or elderly male patient with cervical spine lesion and quadriparesis after minor trauma), lab results, biopsy (pathological confirmation), and imaging findings (the characteristic “mini-brain” sign), the most likely diagnosis is:
Solitary Plasmacytoma of the Cervical Spine (Osseous Plasmacytoma of the Vertebral Body).
If pathological biopsy has confirmed the diagnosis, further differentiation is unnecessary. If there is suspicion of progression or other systemic involvement in the future, evaluation for multiple myeloma is advised.
4. Treatment Plan and Rehabilitation
For patients diagnosed with osseous plasmacytoma, the following treatment and rehabilitation considerations may be applied:
- Treatment Strategy
- Radiation Therapy: For spinal solitary plasmacytoma, local radiation therapy can effectively control the lesion and relieve spinal cord compression. If significant neurological compromise is evident, timely intervention is necessary.
- Surgical Intervention: If there is severe vertebral structural damage or substantial spinal cord compression, or if instability persists after radiation, decompression with internal fixation can be considered to stabilize the spine and relieve pressure.
- Pharmacotherapy: Some patients may require systemic therapy (such as chemotherapy or novel anti-myeloma agents) based on hematologic evaluation to prevent disease progression or transformation into multiple myeloma.
- Rehabilitation and Exercise Prescription
- Rehabilitation Goals: Alleviate limb weakness caused by spinal cord or nerve root compression, enhance cervical spine stability, and prevent secondary muscle atrophy and osteoporosis.
- FITT-VP Principle Example:
- Frequency: Begin with moderate rehabilitation exercises 2-3 times per week in the early stage, gradually increasing to 3-5 times per week as function improves.
- Intensity: Light to moderate intensity (around 50-60% of perceived exertion), avoiding strenuous or rapid head and neck movements.
- Time: 20-30 minutes per session, adjusted based on tolerance. Sessions can be divided into segments, ensuring adequate rest.
- Type: Gentle stretching exercises for the neck and shoulders, light-resistance or isometric exercises for the upper limbs and core muscles, supplemented with basic walking training.
- Volume: Determined by professional assessment of muscle strength and range of motion, with a gradual increase in total exercise volume.
- Progression: As neck and limb strength and endurance improve, incrementally increase training intensity and duration while closely monitoring for pain or neurologic symptoms.
- Safety Considerations: Avoid excessive cervical movement and loading to prevent additional injury. If increased pain, numbness, weakness, or any other discomfort occurs, stop training immediately and seek re-evaluation.
5. Disclaimer
The above analysis is for reference only and does not substitute for an in-person consultation or professional medical advice. Specific treatment and rehabilitation plans should be tailored to the patient’s individual condition and carried out under the guidance of qualified physicians and rehabilitation therapists.
Human Doctor Final Diagnosis
Solitary plasmacytoma involving C5 and C6 vertebrae with "Mini brain"appearance