Bilateral medial oblique menisco-meniscal ligament with medial meniscal tear



Clinical History
A 40-year-old man presented to the accident and emergency department with right knee pain after suffering direct trauma to his right knee after tripping over a low brick wall.
On examination, there was a localised right knee joint tenderness but full range joint movement.
Imaging Findings
The plain radiograph appeared to be within normal limits.
MR imaging demonstrated a horizontal oblique tear in the posterior horn of the left medial meniscus. In addition, bilateral low-signal thin cordlike structures that originated from the anterior horn of the medial meniscus and inserted into the posterior horn of the lateral meniscus were seen. They extended through the intercondylar notch to lie anterior to the posterior cruciate ligament, in keeping with bilateral medial oblique menisci-meniscal ligaments.
Discussion
Background:
Oblique menisco-meniscal ligament (OMML) is an uncommon entity, which has not been extensively described in anatomy or radiology literature. This normal anatomical variant structure is also infrequently mentioned in arthroscopy literature.
It only accounts for 1-4% of all intermensical knee ligaments and its function is poorly understood but thought to contribute in meniscal stability [1-3]. The OMML is named after its anterior attachment site, thus medial oblique menisco-meniscal ligament attaches to the anterior horn of the medial meniscus and posterior horn of the lateral meniscus, while lateral oblique menisco-meniscal ligament attaches to the anterior horn of lateral meniscus and posterior horn of the medial meniscus. Both ligaments pass between anterior and posterior cruciate ligaments as traverse through the intercondylar notch.
Imaging perspectives:
In order to avoid erroneous radiological diagnosis and subsequent unnecessary surgical intervention, it is crucial for radiologists to be familiar with imaging appearances of the OMML when reporting knee magnetic resonance imaging (MRI) due to their resemblance to meniscal tear, in particular to flipped meniscal tear [4-6]. On the sagittal plane imaging this structure could give the appearances of double PCL sign which could be mistaken for an underlying bucket handle tear.
To correctly identify the OMML, one needs to be familiar with the appearances and the course of this structure as it extends from the anterior horn of one meniscus, traversing between both cruciate ligaments, to the posterior horn of the opposite meniscus as it passes through the intercondylar notch. In addition, one must ensure that the adjacent meniscus is of normal morphology at MR imaging in all three imaging planes, with no missing fragments. Once these criteria are met, the oblique menisco-meniscal ligament should be correctly identified at MR imaging as a normal anatomic variation rather than as a displaced meniscal fragment.
Teaching point:
Whilst oblique menisco-meniscal ligament is a rare entity which only accounts for 1-4% of all intermeniscal ligaments, it is pertinent to be aware of its imaging appearances and anatomical course in order to avoid erroneous diagnosis of meniscal tear and subsequent unnecessary surgical intervention.
Differential Diagnosis List
Final Diagnosis
Bilateral medial oblique menisco-meniscal ligaments with left medial meniscal tear
Liscense
Figures
Conventional radiograph of the right knee


Magnetic Resonance Imaging of right knee
Magnetic Resonance Imaging of right knee, sagittal plane

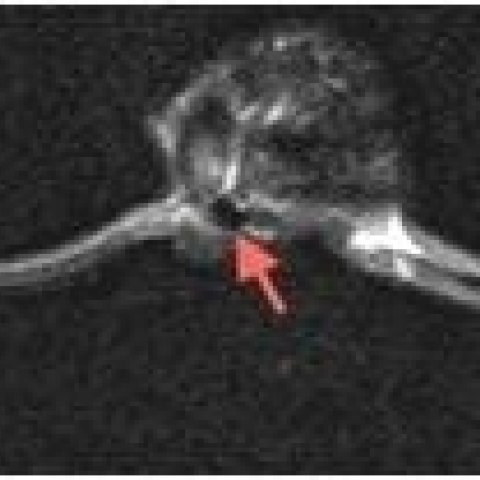
Magnetic Resonance Imaging of right knee, axial plane

Magnetic Resonance Imaging of left knee, coronal plane

Magnetic Resonance Imaging of left knee, sagittal plane


Magnetic Resonance Imaging of left knee, axial plane

Imaging Findings
1. The AP and lateral X-ray views show good continuity of the bony structure in the right knee joint, with no significant narrowing or widening of the joint space, and no clear signs of fracture or dislocation. The patella is in a normal position, and there is no notable swelling of the surrounding soft tissue.
2. MRI sequences reveal a band-like structure within the joint space, originating from the anterior horn of the medial meniscus, running obliquely between the anterior and posterior cruciate ligaments, and attaching to the posterior horn of the lateral meniscus (as indicated by the arrow). Its shape is regular, and the signal intensity is similar to ligament tissue, with no obvious tear signal. In different planes (sagittal, axial, and coronal), this structure appears to have good continuity.
3. Both menisci have intact morphology, with no significant defects or abnormal signals. No flipped meniscus or loose fragment is observed in the anterior or posterior horns. The anterior and posterior cruciate ligaments and collateral ligaments show normal alignment and continuity. No obvious loose bodies or other abnormal signals are seen within the knee joint.
Potential Diagnoses
- Meniscal Tear (such as bucket-handle tear or flipped tear)
Rationale: The patient has a history of trauma, and an apparently "additional band-like structure" on MRI could easily be mistaken for a flipped or loose fragment resulting from a meniscal tear.
Counter-Argument: The MRI actually shows that the meniscus itself maintains normal continuity and morphology, with no local defect signal or flipped tear sign. The observed band-like structure extends obliquely from a portion of one meniscus to the other meniscus, which does not align with a typical meniscal tear. - Oblique Menisco-Meniscal Ligament (OMML)
Rationale: This ligament is found in about 1-4% of all menisco-meniscal ligaments and is often misdiagnosed as a meniscal tear. It can be identified in multiple MRI sequences passing obliquely between the anterior and posterior cruciate ligaments, attaching to the posterior horn of the opposite meniscus—consistent with the typical appearance and location of OMML.
Final Diagnosis
Considering the patient's age and post-injury clinical presentation (only localized knee tenderness, with acceptable range of motion), the absence of clear meniscal or ligament tears on imaging, and the MRI indication of a typical oblique menisco-meniscal ligament structure, the most likely final diagnosis is "Normal Anatomic Variation—Oblique Menisco-Meniscal Ligament", rather than a meniscal tear or other structural damage requiring surgical intervention.
Treatment Plan and Rehabilitation Program
1. Treatment Strategy
· Since the current imaging does not indicate substantial ligament tears or meniscal injuries, and the patient only exhibits localized tenderness, conservative treatment is recommended first.
· Early management follows the RICE principle (Rest, Ice, Compression, Elevation), supplemented by oral or topical NSAIDs to alleviate pain and inflammation.
· If pain worsens or if notable joint locking or mechanical symptoms arise, then further imaging follow-up or arthroscopic evaluation may be considered.
2. Rehabilitation / Exercise Prescription Recommendations
· Early Stage (1-2 weeks):
- Focus on pain relief and reduction of swelling. Perform non-weight-bearing exercises such as straight-leg raises and ankle pumps to maintain basic joint mobility.
- Conduct these exercises 2-3 times per day, each session lasting 10-15 minutes, taking care not to exacerbate pain significantly.
- Within a manageable pain range, progressively increase knee range of motion and muscle strengthening exercises, such as wall squats and seated knee extensions.
- Gradually increase functional training to 2-3 sessions per day, each session lasting 15-20 minutes, with emphasis on strengthening the quadriceps and hamstrings.
- Gradually increase weight-bearing and functional activities, such as partial squats, light step training or stationary cycling, to improve joint stability.
- Adjust exercise intensity based on the patient’s subjective feelings and knee stability, keeping within a safe heart rate range. Training load can be increased by about 10-20% per week to avoid overexertion.
- If the patient is overweight or has osteoporosis, compromised cardiopulmonary function, etc., reduce the impact of exercises and increase rest intervals to avoid excessive fatigue.
- When possible, seek guidance from a professional rehabilitation therapist to develop a personalized training plan and monitor knee status.
Disclaimer: This report is a reference analysis based on the available imaging and clinical information and cannot replace in-person consultation or professional medical advice. Patients should proceed with diagnosis and rehabilitation under professional medical guidance, in alignment with their actual clinical condition.
Human Doctor Final Diagnosis
Bilateral medial oblique menisco-meniscal ligaments with left medial meniscal tear