Morel-Lavallée lesion



Clinical History
An 83-year-old-man returned to the emergency department reporting recent increase of a right thigh tumefaction with years of evolution. He denied recent trauma, pain and fever.
Imaging Findings
Plain films of right thigh (Fig. 1 and 2) revealed a soft tissue lesion in the external surface of the thigh, without significant bone changes.
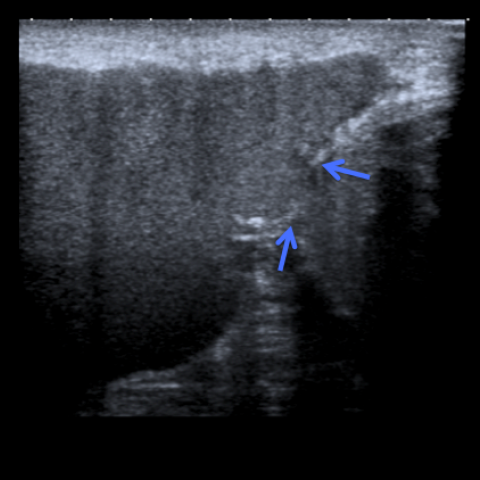
Ultrasound showed a liquefied lesion, surrounded by a capsule with a small area of rupture (Fig. 3 and 4).
MR images (Fig. 5 to 7) confirmed a fusiform lesion, with hematic component between the subcutaneous fat and the underlying fascia. They also confirm the presence of the capsule and the area of its rupture.
Discussion
Morel-Lavallée effusions result from a closed traumatic injury with separation of the interfascial planes between subcutaneous tissue and muscle. [1] The disrupted capillaries drain to the perifascial plane filling the cavity with blood, lymph and debris, which explains the different signal intensity on MRI. Within time, the blood is absorbed and replaced by a serosanguineous fluid, becoming more hyperintense in T1 weighted images. [6]
These lesions are most frequently found around the great trochanter and proximal thigh, although they can also be found in the knee, lumbar region and scapula. [2, 3]
Patients usually present to the hospital in few days after the traumatic event, but up to one third of them can come months or even years later. [4, 6] Symptoms include swelling, bulging, bruising and sensitive changes in the affected area. [2]
Although radiographic studies can show a soft tissue lesion and ultrasound a heterogeneous fluid collection, MR is the modality of choice to evaluate this lesion. [1] This last technique can confirm the diagnosis differentiating it from a soft tissue tumour.
MRI allows also to classify the lesion in one of the six types, according to the shape of the lesion, signal characteristics, the presence or absence of a capsule and enhancement. [5]
Type 1 lesions appear as a laminar shape, with low T1 and high T2 signal intensity. A capsule is usually absent.
Type 2 and type 3 lesions have an oval shape and a thick capsule. The difference between them is that type 2 lesion has high signal intensity in T1 and T2-weighted images, while type 3 has intermediate signal intensity in T1 and heterogeneous in T2 weighted images.
Type 4 has a linear shape and there is no capsule. The signal is usually low in T1 and high on T2-weighted images.
Type 5 is a round pseudo-nodular lesion, with variable signal on T1 and T2-weighted images. The signal intensity in type 6 lesions is also variable, but it is related with infection. Our case represents a type 3 Morel-Lavallée lesion.
In the presence of a history of trauma and in a typical location Morel-Lavallée can be differentiated from tumours.
The therapeutic approach can include aspiration, but it is still under debate because of the possibility of an increased risk of developing overinfection. The preferable treatment is an open drainage and secondary closure. [1]
Our patient was submitted to surgical debridement and primary closure and was discharged two days later fully recovered.
Differential Diagnosis List
Final Diagnosis
Morel-Lavallée lesion of the thigh
Liscense
Figures
Plain film of right thigh

Plain film of right thigh

Ultrasound image

Ultrasound image
T1-weighted image

T1-weighted image

STIR weighted image

Medical Analysis Report
I. Imaging Findings
Based on the multi-directional imaging of the patient’s right thigh (including X-ray, ultrasound, and MRI), the main findings are:
- X-ray findings: Good continuity of the bone around the right femur, with no obvious signs of fracture. A protruding or thickened soft tissue shadow (indicated by the yellow arrow) suggests soft tissue swelling or fluid accumulation.
- Ultrasound findings: A cystic or fluid area can be seen between the superficial fascia and deeper muscle fascia in the right thigh, with uneven internal echoes (indicated by green and blue arrows), suggesting fluid accumulation containing different components (e.g., blood, serous fluid, or mixed debris).
- MRI findings: An elliptical or oval fluid-signal lesion is observed in the proximal anterolateral region of the right thigh. The lesion shows moderate to slightly high signal intensity on T1-weighted images, unevenly increased signal on T2-weighted images, and a thick-walled or capsule-like appearance locally (indicated by the red arrow). These findings are consistent with chronic fluid collection, hematoma, or the typical presentation of a Morel-Lavallée lesion.
II. Potential Diagnoses
Considering the patient’s advanced age (83), the many years of swelling in the right thigh that has recently enlarged, and the imaging findings, the differential diagnoses include:
- Morel-Lavallée lesion (closed degloving injury): Typically presents in the fascial plane where subcutaneous tissue is separated from the underlying fascia. Swelling can appear soon after trauma or many years later. MRI typically demonstrates a cystic or fluid-like mixed signal. The clinical history and imaging are consistent with this diagnosis.
- Soft tissue tumors (e.g., lipoma, liposarcoma): On MRI, these may present as soft tissue masses with characteristic fatty components or tumor-like features, which are not entirely consistent with the thick capsule and mixed blood/serous signal seen in this case.
- Chronic hematoma or cyst: Can form after repeated bleeding from an old injury, but they usually do not exhibit a significant or thickened capsule, and their signals may vary over time based on changes in internal components.
In summary, given the lesion’s location, imaging characteristics, and the patient’s long history of swelling, a Morel-Lavallée lesion is the most likely diagnosis.
III. Final Diagnosis
Based on the patient’s age, the chronic swelling in the right thigh over many years that has recently enlarged, and the MRI findings, the comprehensive judgment is:
The most likely final diagnosis: Morel-Lavallée lesion (Type 3, thick-walled capsule, moderate T1 signal, heterogeneous high T2 signal).
Some cases may still require surgical exploration and operative findings for further confirmation. If there is a high clinical suspicion of malignancy, a biopsy may be performed to rule out other neoplastic processes.
IV. Treatment Plan and Rehabilitation Schedule
Management of a Morel-Lavallée lesion depends on the size, the presence of symptoms, and any infection:
- Conservative treatment: In patients with mild symptoms or small fluid collections, aspiration may be considered, but there is a risk of infection and recurrence.
- Surgical treatment: In cases with large or recurrent fluid collections, open incision, thorough debridement to remove the capsule, and adequate drainage (sometimes combined with negative-pressure wound therapy or other immobilization measures) may be employed to prevent reaccumulation.
Patients generally recover well after treatment, but in elderly patients, overall health status and functional recovery require special attention. Rehabilitation exercises can help reduce adhesions, promote healing, and restore muscle strength. An example exercise prescription is as follows:
- Early recovery phase (1-2 weeks): Focus on isometric contractions of the affected limb and passive joint movements. Avoid high-intensity or excessive activities to prevent wound disruption; perform these 1-2 times per day for 10-15 minutes each time.
- Intermediate strengthening phase (2-4 weeks): Gradually introduce low-load active joint movement exercises (such as flexion and extension in a seated or supine position), along with light resistance training (e.g., using resistance bands) three times a week for 15-20 minutes per session, increasing duration as tolerated.
- Late consolidation phase (4 weeks and beyond): If there is no sign of infection or wound healing complications, progress to moderate-intensity muscle-strengthening and balance training, such as sit-to-stand exercises, short-distance walking, or water-based exercises (which place less impact on joints). Perform these 3-5 times a week, adapting according to tolerance.
Throughout rehabilitation, follow the FITT-VP principle (frequency, intensity, time, type, progression, and individualization). Closely monitor for signs of wound pain, swelling, or fluid reaccumulation. If any significant abnormalities occur, seek medical attention promptly.
Disclaimer: The above analysis is for reference only and cannot replace an in-person consultation or professional clinical judgment. If there are any further changes in symptoms or questions, please consult a specialist or visit a hospital for the appropriate examinations and treatment.
Human Doctor Final Diagnosis
Morel-Lavallée lesion of the thigh