The Geyser sign associated with AC joint cyst



Clinical History
A 87-year-old woman presents with 4 week history of spontaneous, painless and progressive left shoulder swelling.
Physical examination showed a lump on the superior aspect of the shoulder with no evidence of inflammatory signs. Preserved shoulder motion.
Prior medical history included osteoarthritis, rheumatoid arthritis and left shoulder pain.
Imaging Findings
Conventional radiographs showed a soft-tissue mass cranial to the clavicle with central multiple small lucencies and a widened AC joint.
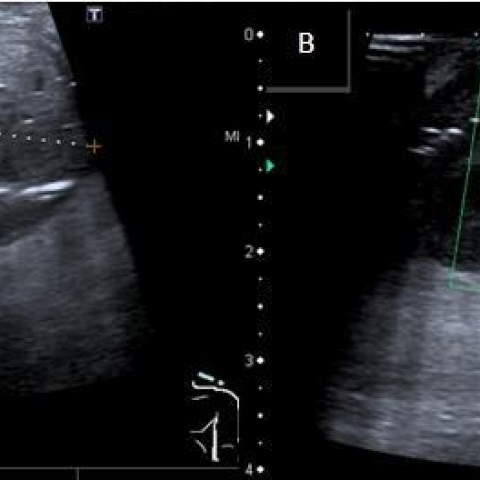
Ultrasound revealed a well-described mass, superior and medial to the acromioclavicular (AC) joint, heterogeneously hypo-echoic with numerous gas artefact images within. No Doppler signal.
MRI showed a full thickness tear of supraspinatus tendon with retraction of the supraspinatus muscle. A soft-tissue mass arising from the glenohumeral joint through the rotator cuff tear and the widened AC joint into the subcutaneous tissue, cranial to the clavicle, was identified (the Geyser sign). Associated muscle atrophy was observed.
The mass had a complex cystic appearance showing intermediate signal intensity on T1 weighted images and heterogeneously high signal intensity on T2 weighted images. After intravenous contrast medium administration peripheral enhancement of the mass was observed. All sequences showed small areas with low signal intensity within the soft tissue mass suggesting gas bubbles.
Discussion
Acromio-clavicular joint (ACJ) cyst is a rare entity, mostly associated as a complication of a massive chronic full thickness rotator cuff tear. Patients tend to be elderly, with significant osteoarthritis of the shoulder [1-4].
The pathogenesis is not entirely understood [4, 5]. It is believed that it has a mechanic aetiology. After a massive rotator cuff tear, the humeral head migrates towards the acromion and therefore impacts repeatedly against the under-surface of the ACJ. This phenomenon produces a capsular joint tear and finally permits the extravasation of synovial fluid from the glenohumeral joint through the osteoarthitic ACJ into the subcutaneous tissue. This chronic process results in cyst formation and therefore progresses until a visible bump develops [1-6].
The patients’ main complaint is a unilateral painless focal mass on top of the shoulder. Clinical examination usually reveals an evident subcutaneous freely mobile mass, over the ACJ rotator cuff tear, in most cases functionally compensated [6].
Conventional radiograph should be the first line of imaging, showing degenerative changes in the glenohumeral joint, associated with soft tissue swelling over the widened ACJ, variable in size and with smooth margins, compatible with a pseudotumour [2-6].
MRI has shown to be an excellent option for excluding a malignant tumour, depicting the cyst and confirming a massive rotator cuff tear. It is also useful to depict the diagnostic pearl called the “Geyser sign” non-invasively, an original fluoroscopic arthrographic finding showing an extravasation of contrast from the glenohumeral joint into the subacromial-subdeltoid bursa through the ACJ, finally extending into the subcutaneous tissue [1-4].
Few cases are reported in the literature, consequently there is limited consensus in its management, varying widely from conservative to surgical [6, 7, 8].
Surgical treatment should be considered to treat the underlying pathology, in most cases the rotator cuff tear, followed by cyst removal, in order to avoid cyst recurrence and improve symptoms [5-7].
In conclusion, ACJ cyst is a rare mechanical complication of a degenerative and massive rotator cuff tear in elderly patients, potentially misdiagnosed as a tumour. Imaging, especially MRI, should be performed to exclude malignancy and make an accurate diagnosis, identifying the "Geyser sign" when present. The aim of the treatment should be primarily to repair the rotator cuff tear, to avoid ACJ cyst recurrence and subsequently to treat the ACJ cyst.
Differential Diagnosis List
Final Diagnosis
ACJ cyst associated with massive degenerative rotator cuff tear.
Liscense
Figures
Antero-posterior radiograph of the left shoulder

Ultrasound of AC joint
T1 and T2 weighted images in sagittal plane

Oblique coronal MRI of the right shoulder. Geyser sign depicted

Medical Analysis Report
I. Imaging Findings
Routine X-ray examination of the patient’s left shoulder shows a reduced distance between the humeral head and the acromion, suggesting an upward migration of the humeral head due to a rotator cuff tear. A soft tissue bulge is visible at the acromioclavicular (AC) joint region, with smooth margins and cystic density changes. MRI indicates a large or full-thickness rotator cuff tear, with cystic fluid signal in the AC joint region that mildly compresses or protrudes locally. The “Geyser sign” is apparent, indicating that contrast or joint fluid has traversed from the glenohumeral joint through the AC joint into the subcutaneous tissue. Overall, these imaging findings are consistent with an AC joint cyst accompanying a large or full-thickness rotator cuff tear.
II. Potential Diagnoses
- AC joint cyst: Commonly found in elderly patients, often caused by chronic or large rotator cuff tears that result in joint fluid leaking into the subcutaneous area around the AC joint. Clinically, it can present as a painless lump on the top of the shoulder.
- Soft tissue tumor or neoplasm: When facing a protrusion or mass on the shoulder, one should consider conditions like synovial tumors or lipomas. However, these usually have distinct imaging and clinical characteristics. MRI can help differentiate malignant or benign tumor-like lesions. Cysts typically appear as uniform fluid signals on MRI.
- Bone spur or cartilaginous exostosis (e.g., osteophytes): Bony joint changes can lead to proliferative lesions in the AC joint, typically showing high-density bony findings rather than a clear-cut cystic manifestation.
Based on the cystic bulge observed at the top of the shoulder, the MRI findings of fluid accumulation in the AC joint area against the background of a rotator cuff tear, along with the “Geyser sign,” an AC joint cyst is the most likely diagnosis.
III. Final Diagnosis
Considering the patient’s advanced age, a known chronic rotator cuff tear (or risk factors such as rheumatoid arthritis or degenerative joint disease), and the imaging evidence of a typical cystic protrusion, the most likely diagnosis is: AC joint cyst secondary to a massive rotator cuff tear.
IV. Treatment Plan and Rehabilitation Program
According to current research and literature, the primary treatment focus is repairing the rotator cuff tear to prevent the cyst from persisting or recurring. Specific treatments can be categorized into:
- Conservative treatment: If the patient has mild symptoms with acceptable overall function, conservative measures may be considered. These include local physical therapy (e.g., physiotherapy, ice or heat application), functional training, and appropriate use of analgesics and anti-inflammatory medications.
- Surgical treatment: In cases of a clearly identified large/full-thickness rotator cuff tear causing significant functional impairment or a visibly prominent cyst with risk of rupture, arthroscopic or open surgical repair of the rotator cuff and excision of the cyst may be performed to reduce recurrence and improve function.
Rehabilitation/Exercise Prescription can follow the FITT-VP principles:
- Frequency (F): Perform shoulder rehabilitation exercises at least 3–5 times a week.
- Intensity (I): Begin with low-intensity exercises (within a pain-tolerable range of motion). Focus on active range-of-motion exercises for the shoulder in various directions. Gradually introduce low-resistance training, such as elastic band or light dumbbell exercises, in later stages.
- Time (T): Start with 10–15 minutes per session and increase gradually up to around 30 minutes as tolerated.
- Type (T): Emphasize range-of-motion and rotator cuff muscle strengthening exercises (external rotation, internal rotation, forward flexion, abduction), either actively or with assistance.
- Progression (P): As shoulder strength and stability improve, progressively increase resistance and range of motion, but avoid excessive overload.
If the patient has osteoporosis or reduced cardiopulmonary function, it is crucial to adjust exercise intensity and frequency under professional supervision to minimize the risks of falls and other complications.
Disclaimer: This report is for reference only and does not replace in-person consultations or professional medical advice. If you have any discomfort or questions, please consult a specialist or visit a medical facility promptly.
Human Doctor Final Diagnosis
ACJ cyst associated with massive degenerative rotator cuff tear.