Anterior cruciate ligament tear due to impingement from bony outgrowth



Clinical History
Patient presented with right knee joint instability without any history of trauma. The symptoms were more pronounced while walking down the stairs, with an onset of 5 years prior to imaging. On physical examination, both the pivot shift and the Lachman’s tests were positive for anterior cruciate ligament (ACL) tear.
Imaging Findings
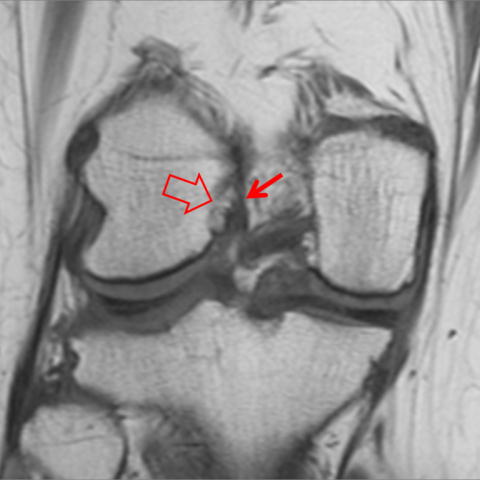
The axial T2-w, coronal T1-w and sagittal PD-w MR images (Fig. 1-3), showed a bony outgrowth at the medial aspect of the lateral femoral condyle projecting into the intercondylar notch. The ACL was horizontally displaced and torn. Moderate joint effusion was also evident.
Discussion
A. The ACL is a stabilizer of the knee that resists anterior translation and secondarily resists varus and valgus forces. ACL tear usually occurs following a quick deceleration, hyperextension or rotational injury. Very rarely, the ACL may be torn due to its impingement against the intercondylar notch.
B. An acute ACL tear following trauma is characterized by pain, haemarthrosis and instability. At the time of injury, a popping sound or sensation may occur. The role of MRI is to explore the presence of ACL rupture and in addition to show any associated findings such as meniscal tears and osteochondral injuries.
C. The MRI findings in ACL tears include discontinuation, swelling, and horizontal course [1]. Non-traumatic ACL tears may result from a mal-positioned screw after ACL reconstruction and in non-operated patients from intecondylar notch disorders such as narrowing, enthesophytes and congenital bony outgrowth [2].
D. A torn ACL in a young symptomatic adult should be treated with arthroscopic reconstruction. MRI is necessary to confirm the ACL tear and reveal any additional pathology. In our case, it showed in addition the presence of a bony outgrowth, which allowed the proper treatment planning that included removal of the extra bone.
E. ACL rupture in non-injured patients may result from chronic impingement causing ligamentous degeneration. MRI is the imaging method of choice for exploring this underlying cause.
Differential Diagnosis List
Final Diagnosis
ACL tear due to chronic impingement from bony outgrowth
Liscense
Figures
Axial T2-w MR

Coronal T1-w MR
Sagittal PD-w MR

I. Imaging Findings
Based on the provided MRI images, the following main features are observed:
- The anterior cruciate ligament (ACL) shows discontinuity with local signal irregularities, suggesting disruption of its fiber integrity.
- A noticeable bony protrusion or abnormal osseous overgrowth is present in the femoral intercondylar notch region adjacent to the ACL, which may cause mechanical impingement or compression of the ligament.
- No obvious fracture signs due to acute injury are observed inside the joint; however, joint effusion or mild soft tissue edema may be present.
- The articular cartilage surface appears essentially intact overall. Further evaluation is recommended to check for meniscal injury; if clearer imaging sequences are available, potential occult meniscal tears or cartilage damage should also be considered.
II. Potential Diagnoses
- Anterior Cruciate Ligament Tear (Non-Traumatic/Chronic Impingement Injury)
Characteristics: The patient has no clear history of acute trauma but experiences joint instability symptoms; MRI shows ACL discontinuity or abnormal course. Such chronic damage may be related to repeated impingement from a bony protrusion in the femoral intercondylar notch. - Degenerative Partial Tear of the ACL
Characteristics: This is relatively uncommon in younger individuals, but it can occur on the basis of ligamentous degeneration, showing fiber disorganization, abnormal signals, and partial tear. Local bony overgrowth in the intercondylar notch can further exacerbate wear and tear. - Combined or Isolated Meniscal Injury
Characteristics: Some patients with chronic ACL injury may also have meniscal degeneration or instability-related meniscal tears. However, the current imaging does not clearly indicate significant meniscal tears. Further detailed imaging sequences and clinical examinations are required to rule this out.
Based on the patient’s symptoms (aggravated instability when descending stairs), physical examination (positive Lachman and Pivot Shift tests), and the MRI findings of disrupted ligament integrity, an ACL tear is the main concern.
III. Final Diagnosis
Considering the patient’s age, clinical presentation (knee instability without obvious trauma), positive physical exam, and imaging findings, the most likely diagnosis is:
“Non-traumatic (Chronic Impingement) ACL Tear Combined with Abnormal Bony Overgrowth in the Femoral Intercondylar Notch.”
This bony overgrowth or prominence may lead to repeated ligament impingement and wear, resulting in chronic ACL tear.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategies
- Surgical Treatment: The goal is to restore joint stability and function. Arthroscopic removal of the abnormal bony protrusion can be considered to reduce mechanical impingement on the ACL. If the ligament damage is extensive, ACL reconstruction surgery (commonly using an autologous tendon graft) may be necessary.
- Conservative Treatment: For early or mild symptoms, combining a knee brace and physical therapy aims to reduce the feeling of instability. However, given the pronounced instability in this case, surgical intervention usually provides a better outcome.
2. Rehabilitation/Exercise Prescription Recommendations
The rehabilitation plan should follow a gradual progression (FITT-VP principle). The detailed steps are as follows:
- Preoperative or Acute-Phase Rehabilitation
- Goal: Alleviate pain, protect the joint, and prevent muscle atrophy.
- Content: Use a knee brace to stabilize the joint; perform isometric quadriceps exercises (e.g., straight leg raises) within a pain-free range.
- Frequency and Progression: 1–2 times daily, with each session adjusted based on tolerance. Avoid large-range joint movements and excessive weight-bearing.
- Early Postoperative Phase (0–2 weeks)
- Goal: Reduce swelling and maintain stability of the ligament graft or repair.
- Content: Continue using a brace, perform ankle pump exercises, isometric quadriceps training, and non-weight-bearing knee range of motion (restricting flexion-extension to a safe range).
- Frequency and Progression: 2–3 times daily, 5–10 minutes each session, with adjustments according to wound healing and swelling.
- Mid Postoperative Phase (2–6 weeks)
- Goal: Restore knee joint range of motion and improve muscle strength.
- Content: Gradually increase the range of flexion-extension, use a balance board for light balance training, and perform active resisted strengthening of the quadriceps and hamstrings. Transition to partial weight-bearing ambulation.
- Frequency and Progression: 3–5 times per week, 20–30 minutes each session. Monitor the knee’s response closely and gradually increase training resistance as tolerated.
- Late Postoperative Phase (6 weeks–3 months and beyond)
- Goal: Fully restore muscle strength and joint stability to prepare for daily activities and sports.
- Content: Gradually increase lower limb weight-bearing exercises, use a stationary bike, do resistance band squats to enhance lower limb strength and proprioception; attempt light jogging or directional changes under professional guidance.
- Frequency and Progression: 3–5 times per week, increasing intensity and duration in line with functional improvement. Ensure proper technique to avoid re-injury.
Throughout the rehabilitation process, training intensity and methods should be adjusted dynamically based on the patient’s individual condition (bone quality, cardiopulmonary function, pain level). Regular follow-up and professional input are crucial, and additional imaging assessment may be required if necessary.
Disclaimer:
This report is a preliminary analysis based on current imaging and clinical information. It is intended for medical reference and cannot replace in-person consultation or the advice of a professional physician. Specific treatment and rehabilitation plans should be carried out under the guidance of an orthopedic or sports medicine specialist.
Human Doctor Final Diagnosis
ACL tear due to chronic impingement from bony outgrowth