Surgical management of rickets



Clinical History
A 52-year-old lady with known history of hypophosphataemic rickets was referred complaining of increasing pain and decreased ability to weight bear.
She presented initially at age 35 with bilateral knee pain. She had a high tibial osteotomy at the age of 37 and then removal of metal work at 46.
Imaging Findings
The lateral image shows she is developing a transverse stress fracture at the junction of the middle and distal 1/3 of the femur.
The femur radiograph shows a varus deformity and a developing fracture in the middle 1/3 and proximal 1/3. A pseudofracture is also present on the medial aspect of the femur in the subtrochanteric area – a Looser’s zone.
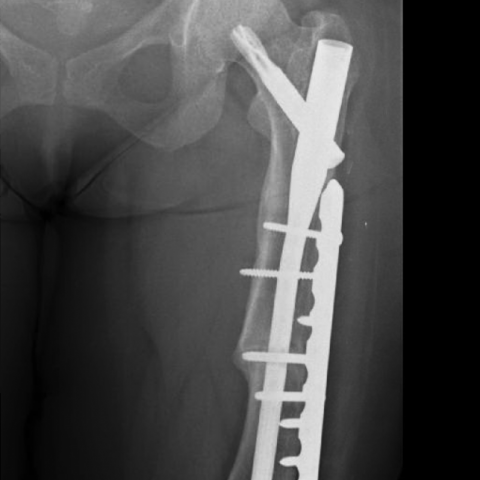
18 months post-operative films show the IM nail in correct position and bony union at the osteotomy site.
Discussion
X-linked hypophosphataemic rickets is an x-linked dominant form of rickets that can cause short stature and genu varum (bow-leggedness).
It is due to mutation of the PHEX gene, which causes inactivity of the PHEX protein [1]
Prevalence of this condition is 3.9-5 per 100, 000 live births [2].
Looser’s zones are pseudofractures. They are wide transverse lucencies that traverse partially across a bone, usually at right angles to the involved cortex [4].
Looser’s zones can be seen in a variety of conditions including osteomalacia, renal osteodystrophy, Paget’s disease of the bone, osteogenesis imperfecta and rickets [4].
It was evident from the radiographs of the femur that this patient had Looser’s zones on the medial aspect of the femur and a significant varus femoral deformity. As a result, a stress fracture was also visible affecting the lateral femoral cortex. Due to her increasing symptoms and the appearance of the area on the lateral cortex, it was felt appropriate to intervene before the bone fractured.
Treatment of hypophosphataemic rickets can involve oral phosphate, calcitriol and if bowing is severe such as in this case, an osteotomy may be performed to improve alignment of the leg [3].
The patient underwent intramedullary nailing of the left femur with a wedge osteotomy and plating to allow adequate healing with realignment of the femur. Subsequent radiographs showed bony union and, along with an improved clinical picture, proved the successful management of this condition.
Differential Diagnosis List
Final Diagnosis
Looser’s Zones/pending stress fracture secondary to rickets
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Lateral femur

AP femur

18 month post op

1. Radiological Findings
Based on the submitted lower limb X-ray images and the patient's clinical data, the following can be observed:
- A transverse radiolucent band is visible on the medial side of the mid-distal femoral shaft, presenting as Looser’s zone (pseudofracture).
- Signs of a stress fracture are present in the lateral cortex, which is associated with repetitive lower limb loading and poor bone quality.
- There is evident imbalance of stress in the medial and lateral cortex of the femoral shaft, leading to local deformity and stress concentration.
- Postoperative images show intramedullary nail fixation of the femoral shaft, along with wedge osteotomy correction and plate-screw fixation. There are clear signs of fracture/pseudofracture healing, and the internal fixation is in good position.
2. Potential Diagnosis
Given the patient’s history of “low-phosphorus rickets (X-linked hypophosphatemic rickets),” along with the presence of Looser’s zone and stress fractures, the following diagnoses should be considered:
- X-linked hypophosphatemic rickets: Caused by a mutation in the PHEX gene, resulting in hypophosphatemia. It often presents with skeletal deformities (e.g., genu varum, short stature), and imaging may show osteomalacia and Looser’s zones.
- Osteomalacia (e.g., due to vitamin D deficiency): May present with similar occult fractures (Looser’s zones). However, in this case, a definitive diagnosis of X-linked hypophosphatemic rickets and long-term history more adequately explains the lesions.
- Other rare metabolic bone diseases: Such as renal osteodystrophy, osteoporosis, etc. These can also present with pseudofractures or stress fractures. However, the specific genetic background and clinical presentation in this patient make these less likely.
3. Final Diagnosis
Based on the patient’s history of hypophosphatemic rickets, typical presentation of Looser’s zone (pseudofracture), signs of stress fracture, and radiographic evidence of healing after surgical fixation, the most likely final diagnosis is:
- X-linked hypophosphatemic rickets with femoral stress fracture (Looser’s zone)
4. Treatment Plan and Rehabilitation Program
4.1 Treatment Strategies
- Pharmacotherapy: Oral phosphate supplements and active vitamin D (e.g., calcitriol) to correct hypophosphatemia and stabilize bone metabolism.
- Surgical Correction and Internal Fixation: For patients with severe skeletal deformities or at risk of stress fractures, as in this case, osteotomy, intramedullary nailing, or plating can be performed to facilitate fracture healing and improve alignment.
- Regular Follow-up: Postoperatively, regular X-ray evaluations should be conducted to monitor fracture healing and the outcome of correction procedures, as well as to assess serum phosphate, calcium, and other indicators for timely medication adjustments.
4.2 Rehabilitation and Exercise Prescription
Rehabilitation must be tailored to the patient’s bone quality and surgical recovery status, following a gradual and individualized approach. The recommendations are as follows:
- Early Stage after Removing or Reducing External Fixation (0-6 weeks post-op):
- Focus primarily on passive or assisted active movements of the affected limb to reduce joint stiffness and muscle atrophy.
- Isometric contractions of the quadriceps and peri-hip muscle groups can be performed while seated or under low load (holding each contraction for 5-7 seconds, resting 5 seconds, repeating 10-15 times, 2-3 sets daily).
- Gradually progress to partial weight-bearing training with orthotic support. The initial walking duration can be limited to a few minutes, adjusting according to pain and fatigue.
- Mid-stage Rehabilitation (6-12 weeks post-op):
- If the fracture shows good progression in healing, gradually increase weight bearing and begin walking with handrail support or assistive devices.
- Resistance band exercises can be added to strengthen the quadriceps, hamstrings, and hip muscles. It is recommended 2-3 times per week for 20-30 minutes each session.
- If feasible, perform aquatic walking or cycling in a pool to reduce joint stress.
- Late-stage Rehabilitation (12 weeks post-op and beyond):
- Once bone healing is sufficient and muscle strength and range of motion have recovered well, gradually transition to normal gait training without orthoses or assistive devices.
- Incorporate core and lower limb integrated exercises (e.g., seated cycling, brisk walking on level ground, step training), about 30 minutes per session, 3-4 times per week.
- Depending on the patient’s bone condition and cardiopulmonary status, modest strength training or light jogging can be considered. Close attention should be paid to avoid fatigue and ensure safety throughout.
Throughout rehabilitation, closely monitor symptoms such as pain and swelling. If there is significant discomfort or new symptoms, seek medical evaluation promptly.
5. Disclaimer
This report is based on the current imaging and clinical information for preliminary analysis. It is intended for reference only and cannot replace in-person consultations or professional medical advice. If you have any questions, please consult your attending physician or visit a hospital for further evaluation.
Human Doctor Final Diagnosis
Looser’s Zones/pending stress fracture secondary to rickets