


A 10 year old girl presented with continous pain in her left ankle after a sprain history.
Radiographs of her left ankle demostrate lytic lesions with sclerotic component, adyacent to the physis.
Laboratory test were normal. Histological findings and cultures of two previous percutaneous biopsies were inconclusive.
Radiographs(Anteroposterior and lateral proyections of both ankles and Anteroposterior proyection of both Knees) revealed predominant lytic lesions with peripheral sclerotic halo, adyacent to the physis and symmetrical involvemente of both ankles and knees(Fig 1-3).
Radiographs of the chest showed expansion and periostal reaction on the posterior aspect of the 3th right rib(Fig 4).
Magnetic resonance imaging(MRI) of the left ankle demostrated a medullary lesion with peripheral sclerosis and multiple patchy and coalescent areas isointense on T1 and hyperintense on T2 weighted images. It was also observed soft tissue edematous changes(Fig 5-7).
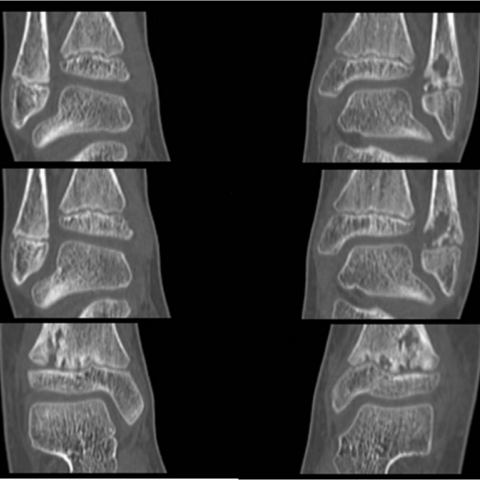
CT showed cortical bone thickening with irregular contours and multiple, partly confluent osteolytic foci(Fig 8).A biopsy of the distal left tibia region was obtained and showed a highly vascularised, predominant inflammatory process with bone resorption and apposition. Malignancy could be excluded. Molecular biologic studies and cultures were negative for bacteria.
The diagnosis of CRMO was established.
Chronic recurrent multifocal osteomyelitis (CRMO) is an idiopathic inflammatory skeletal disorder of children and young adults that is characterized by multifocal non pyogenic inflammatory bone lesions [1].
The cause remains unknown though recently a genetic component has been suggested. Its association with skin lesions or inflammatory bowel disease is well documented [1, 2]. There is also a close link with SAPHO syndrome (Synovitis, Acne, Pustulosis, Hyperostosis and Osteitis). By some authors, SAPHO is regarded as the adult form of CRMO and vice versa [2].
The onset of clinical symtomps is often insidious and non specific with exacerbations and remissions. Systemic manifestations such as fever, weight loss and lethargy may be present but are unusual. Laboratory tests may be normal, and pain is typically localised, even in a multifocal disease [1].
Most cases (up 85%) occur in children (average age of 10 years) with female predominance. Lesions typically involve the methaphyses of tubular bones with predilection for the lower extremities, followed by the clavicle, spine, ribs, mandible and pelvis [1, 3].
Symmetric involvement is common and multifocality is virtually always present [3, 4].
Radiological and histopathological findings of CRMO are similar to chronic infectious osteomyelitis which initially appears on radiography as lytic destruction within the methaphysic area adjacent to the physis, demarcated by a thin sclerotic rim. These inflammatory changes may progress to involve the diaphysis with periosteal new
bone formation [3-5]. During new exacerbations, small lytic lesions and periosteal new bone formations appear as signs of activity. In the reparative disease phase, areas of metaphyseal and epiphyseal destruction healing with sclerosis are present [3, 5].
MRI is highly sensitive to diagnose hidden lesions and extremely accurate to evaluate disease activity and local extent, and helpful for biopsy guidance and evaluation of long-standing disease. Active disease appears as areas of high signal on T2WI or STIR images, and decreased signal intensity on T1-WI. Quiescent disease correlates with low signal on T1 and T2 WI images, corresponding to sclerosis, possibly with scattered areas of high signal related to fatty marrow.
Histophatology is that of non specific inflammation, with fibrosis and/or hyperostotic regeneration [5, 6].
CRMO is a diagnosis of exclusión and differention diagnosis mainly includes infectious osteomyelitis and tumour or tumour-like lesions. Biopsy is needed to exclude malignant disease [1, 2, 4-6].
CRMO is generally a self-limiting disease, however up to the 50% of patients may experience skeletal growth disturbances or deformities later in life [4, 5]. Radiologists should be familiar with the typical imaging findings of CRMO to prevent unnecessary multiple biopsies and long-term antibiotic treatment [1, 4-7].
Chronic Recurrent Multifocal Osteomyelitis.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.







This patient is a 10-year-old female with a prolonged history of pain around the left ankle joint, initially triggered by a sprain, followed by persistent pain. A comparison of X-ray images reveals a radiolucent area (lytic lesion) near the metaphysis of the distal tibia, surrounded by a certain degree of sclerotic rim. The cortical bone does not show obvious disruption. MRI sequences (including T1WI and T2WI/STIR) demonstrate a high-signal area within the bone marrow, partly accompanied by marginal sclerosis and a low-signal band, irregularly distributed, suggesting local bone marrow edema or inflammatory changes. No significant soft tissue mass or notable abscess is observed, and the distal joint space relationship remains essentially normal.
Further examinations likewise indicate that the distal metaphysis or adjacent metaphyseal region of the tibia and fibula repeatedly display small lytic lesions and mild sclerotic changes. Similar findings have been reported in other locations (e.g., knee joint, clavicle, etc.). Two previous biopsy and bacterial culture attempts did not confirm any specific pathology or infectious pathogen. Routine blood counts and inflammatory markers appear generally normal.
Considering the patient’s age (10-year-old female), clinical history (recurrent lesions in multiple sites but negative lab results and biopsy), imaging characteristics (metaphyseal lytic lesion in the distal tibia with a sclerotic rim and MRI signs of inflammatory edema), and the exclusion of other potential diagnoses, the most likely diagnosis in this case is:
Chronic Recurrent Multifocal Osteomyelitis (CRMO).
If there is still doubt regarding the diagnosis, it would be advisable to observe for recurrent episodes of flare-up and remission, and to consider imaging follow-up or repeat biopsy (to exclude tumor or infection). However, given the current evidence, CRMO appears most consistent.
Treatment Strategy:
Rehabilitation/Exercise Prescription:
Rehabilitation should follow a gradual progression principle (FITT-VP: Frequency, Intensity, Time, Type, Volume, and Progression), carefully accounting for bone involvement risk and the patient’s growth needs.
Throughout the rehabilitation process, monitor any recurrence or exacerbation of local pain, swelling, or other discomfort. If such signs appear, adjust the rehabilitation intensity or seek medical evaluation promptly.
This report is based on current clinical and imaging data for reference purposes only and does not replace an in-person consultation or professional medical advice. If you have any questions or if the condition changes, please consult orthopedics, radiology, or other relevant specialists for further evaluation.
Chronic Recurrent Multifocal Osteomyelitis.