Multiple tendon xanthomas in a child with familial hypercholesterolaemia



Clinical History
A 10-year-old boy presented with the complaint of gradually progressing swelling around the right knee for 1 year. On physical examination, the quadriceps and patellar tendon of the right knee were bulky. Thickening was also noted in quadriceps and patellar tendon of left knee and bilateral achilles tendons.
Imaging Findings
Ultrasonography with panoramic imaging of extensor tendons of bilateral knee and bilateral achilles tendons was performed.
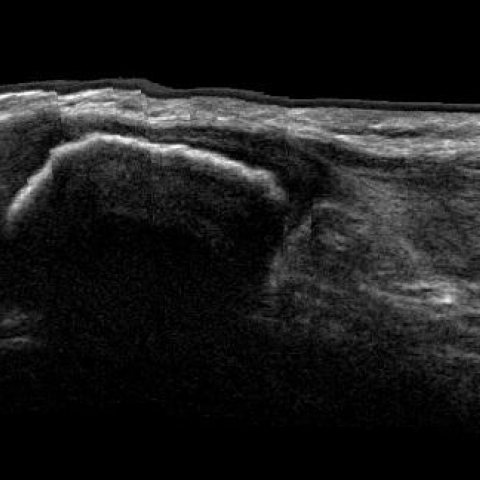
Diffuse fusiform thickening of the tendons was noted with loss of normal fibrillary architecture. There was loss of concavity of the inner margins of both achilles tendons with convex inner margins. The affected tendons show heterogeneous nodular architecture.
Bilateral elbows, hands and wrists were also evaluated by ultrasound but did not reveal any abnormality.
Imaging features were suggestive of multiple tendon xanthomas and hence, lipid profile was advised. The serum cholesterol, serum Low Density Lipoprotein (LDL) cholesterol and serum triglycerides were 894mg/dl, 619mg/dl and 184mg/dl respectively.
Fine needle aspiration cytology from achilles tendon was done and was diagnostic of xanthoma.
Discussion
Xanthomas are small lumps located in the skin or subcutaneous tissue that consist of cholesterol, cholesterol esters, triglycerides, phospholipids and numerous lipid-laden foamy macrophages. The most frequent site is the achilles tendon [1]. Xanthomas are commonly seen in familial hyperlipidaemias type 2 and 3, but could also be associated with non-familial hypercholesterolaemia, drug-induced hypercholesterolaemia and cerebrotendinous xanthomatosis [2]. As the xanthomas enlarge, they can cause pain, restricted joint mobility, disability, and tendon rupture [3, 4].
Xanthomas may precede the diagnosis of hyperlipidaemia, hence early identification can lead to preventative treatment that reduces the risk and morbidity of cardiovascular disease, including myocardial infarction.
Although physical examination may reveal achilles tendon xanthomas, there are several imaging methods for their detection with ultrasonography being the method of choice in everyday clinical practice. Normal sonographic appearance of tendons is characterised by multiple parallel linear echoes that give a fibrillar pattern. Xanthomas have been described either as hypoechoic nodules or as having a diffusely heterogeneous echo pattern at sonography [1]. Partial tendon tears or tendinitis may present a similar appearance and may cause wrong diagnosis. In our patient, sonography revealed diffuse fusiform thickening of tendons of knee and ankle with altered echotexture and multiple hypoechoic nodules.
MRI of the tendon xanthomas demonstrates morphological and signal intensity abnormalities. When a xanthoma is present, the normally flat or concave margins of tendons may change and may have a convex appearance on axial images. Also, the tendons tend to have higher signal intensity on T1-weighted and T2-weighted spin-echo images than normal tendons do [5, 6].
Although several treatments for achilles tendon xanthomas have been proposed, they target mostly the treatment of the basic metabolic disorder of lipid metabolism, which is the main cause of these lesions. Surgery is reserved for larger lesions, often associated with symptoms.
Differential Diagnosis List
Final Diagnosis
Multiple tendon xanthomas in a child with familial hypercholesterolaemia
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Right achilles tendon

Left achilles tendon

Right knee sagittal panoramic view

Left knee sagittal panoramic view
Right patellar tendon short axis

Medical Imaging Analysis Report
1. Imaging Findings
Based on the provided ultrasound images and the patient’s clinical information, the main findings are as follows:
- Marked diffuse thickening of the tendons around both knees, especially in the quadriceps tendon and patellar tendon regions, appearing fusiform in shape.
- Within the thickened tendons, the echo texture is relatively heterogeneous, and multiple hypoechoic or anechoic small nodules can be observed locally, showing “plaquelike” or “nodular” changes.
- Both Achilles tendons also present similar diffuse thickening and abnormal echoes.
- No obvious bone destruction or abnormal changes in the bone were found.
These findings suggest a possible infiltrative or depositional lesion involving the tendons or their insertion sites.
2. Potential Diagnoses
Based on the patient’s age, symptoms, and imaging characteristics, the following potential or differential diagnoses should be considered:
- Tendon Xanthoma: Commonly associated with familial or secondary hyperlipidemia, presenting as lipid deposits in tendons and ligaments. On ultrasound, they appear as fusiform thickening with low or mixed echogenic nodular deposits.
- Tendinopathy or enthesopathy (such as chronic tendonitis): Tendons may show thickening and heterogeneous echogenicity, but typically present with local pain or inflammatory changes and may not always have multiple nodular hypoechoic areas.
- Lipoma or other soft tissue masses: Usually display relatively homogeneous fatty echogenicity on ultrasound, often with a well-defined border; less likely to present as multiple scattered nodules within the tendon.
- Other infiltrative metabolic diseases: Such as gouty tophi. However, gouty lesions commonly appear in adults, often as hyperechoic foci or with calcifications, which do not match the findings in this case.
3. Final Diagnosis
Considering the patient’s age, clinical presentation (bilateral symmetrical tendon thickening and nodular changes), ultrasound features, and possible association with familial or secondary hyperlipidemia, the most likely diagnosis is:
Tendon Xanthomas
To further clarify the underlying cause, it is recommended to obtain a complete lipid profile (including TC, LDL-C, HDL-C, triglycerides, etc.) to assess for familial hyperlipidemia or other forms of secondary hyperlipidemia.
4. Treatment Plan and Rehabilitation Program
4.1 Treatment Strategy
- Lipid Management: If the patient is diagnosed with familial or other hyperlipidemia, lipid-lowering medications (e.g., statins) should be used under pediatric or endocrinology guidance, combined with dietary control and lifestyle modifications.
- Local Treatment: For tendon xanthomas without significant functional impairment or pain, conservative management and follow-up are generally preferred. If there is obvious pain, functional limitation, or a large mass affecting joint movement, surgical excision may be considered.
- Nutrition and Lifestyle: Follow a low-fat, balanced diet, avoid excessive sugar and saturated fats, and maintain a healthy body weight.
4.2 Rehabilitation and Exercise Prescription
In early or mild stages of the condition, a gradual, individualized rehabilitation strategy is recommended.
- Training Goals: Maintain joint range of motion, enhance tendon elasticity and strength, and reduce the risk of tendon injury.
- Exercise Methods:
- Gentle range-of-motion exercises (active or passive stretching), such as straight leg raises and quadriceps strengthening exercises.
- Low-impact aerobic activities, such as swimming or cycling, to minimize stress on the knee joints and Achilles tendons.
- Progressive resistance exercises with low weight and higher repetitions, focusing on improving lower-limb muscle strength and endurance.
- FITT-VP Principle (Example):
- Frequency: 3-4 sessions per week, with rest days as needed.
- Intensity: Low to moderate intensity (RPE 3-4), gradually increasing according to the patient’s condition.
- Time: 20-30 minutes per session, which can be divided into segments.
- Type: Combined gentle joint mobility work, light resistance training, and aerobic activities.
- Progression: Gradually increase exercise intensity and duration as the tendons adapt and symptoms improve.
- Precautions: If pain worsens or discomfort occurs, discontinue activity and seek medical evaluation. Patients with hyperlipidemia or cardiovascular concerns should exercise under professional guidance in a stepwise manner.
5. Disclaimer
This report is a reference analysis based on the current imaging and clinical information. It does not replace an in-person evaluation or a diagnosis and treatment plan made by a professional physician. Specific treatment and rehabilitation plans should be tailored to the patient’s actual condition and carried out under the guidance of a qualified medical professional.
Human Doctor Final Diagnosis
Multiple tendon xanthomas in a child with familial hypercholesterolaemia