Pelvic bone giant cell tumour



Clinical History
A 55-year-old woman presented with pain in the left groin region.
Imaging Findings
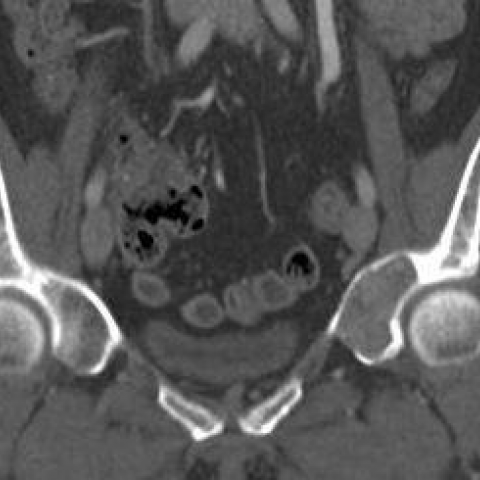
An expansile geographic lytic lesion with a narrow zone of transition and cortical thinning was found involving the left acetabulum.
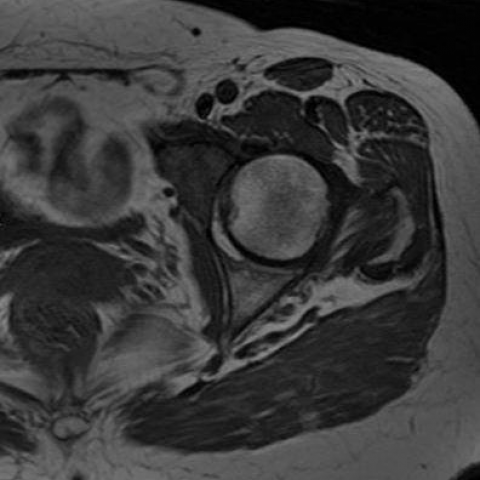
On MR images, the lesion showed predominantly low signal intensity at the T1 and T2-weighted images. No cystic component nor fluid-fluid levels were noted. Solid enhancement was seen after Gadolinium-Based Contrast Media administration.
Discussion
Giant cell tumour of bone (CGTB) is a relatively rare, usually benign, bone tumour, that can be locally aggressive and even metastasize to the lungs. They are typically solitary [1].
The vast majority of lesions occur after physeal closure and are typically seen in young adults, between 20 and 50 years of age [1].
Most of the tumours develop at the end of the long bones but may also occur in flat bones and apophysis [2].
Pelvic location is relatively rare, with the acetabulum appearing the commonest site [3].
CGTB consists of numerous multinucleated osteoclastic giant cells uniformly distributed amongst a proliferation of mononuclear stromal cells that express RANKL, which appears to be play an important role in the pathogenesis of these lesions. Tumours often contain haemorrhagic areas [2].
The typical imaging appearance is a geographic lytic lesion with a well-defined margin without surrounding sclerosis, often with mild bone expansion. The lesion typically abuts the articular surface. More aggressive features such as broader zone of transition, cortical thinning, cortical break-through and soft-tissue mass can also be present. There is no matrix calcification [1].
The degree of aggressiveness by imaging does not correlate with histology and does not appear to predict well either the risk of local recurrence or the development of lung metastases.
On T2-weighted images areas of low signal intensity are typically seen due to large amounts of haemosiderin, fibrosis or high cellularity [1].
Fluid-fluid levels might be seen due to secondary aneurysmal bone cyst (ABC) component, which has been reported in 14% of cases [4].
The presence of enhancing solid components helps differentiate CGTB with secondary ABC from primary ABC [1].
Surgery is the treatment of choice for resectable tumours. In general, intralesional curettage is usually recommended. Combination of curettage with bone cement (polymethylmethacrylate, PMMA) increases local control [5, 6].
In conclusion, GCTB shoud be considered in the differential diagnosis of pelvic bone lytic lesions, particularly when meeting the aforementioned epidemiologic and imaging features.
Differential Diagnosis List
Final Diagnosis
Pelvic bone giant cell tumour
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Pelvis with bilateral hip joints radiopraph:

Multislice CT coronal reformatted image:
Axial MR images:

Axial FST1-weighted MR images:


Medical Imaging Analysis Report
I. Radiological Findings
1. X-ray (Pelvic AP View): A relatively well-defined, lytic “geographic” lesion is observed in the left acetabulum (iliac bone). There is only slight expansion, with no obvious sclerotic rim, and no notable calcification or intraosseous formation.
2. CT (Coronal View): A large, low-density bone defect is seen in the left acetabular region. The lesion has a well-defined contour, locally thinned cortical bone, and mildly compressed adjacent soft tissue. There may be a slight protrusion of soft tissue component, but no obvious calcification.
3. MRI: On T1-weighted images, the lesion appears as medium to slightly low signal intensity in the left acetabulum. On T2-weighted images, parts of the lesion show low signal intensity, suggesting possible hemorrhage, hemosiderin, or fibrous content. A small amount of fluid-fluid levels is visible, suggesting changes similar to aneurysmal bone cyst (ABC) internally.
4. Post-contrast enhancement shows marked enhancement in the solid portion of the lesion, consistent with a lesion predominantly composed of mononuclear stromal cells mixed with vascularized or cystic areas. No significant evidence of distant metastasis is identified.
II. Differential Diagnosis
1. Giant Cell Tumor of Bone (GCTB):
- Commonly seen in adults with closed epiphyseal plates through middle age (approximately 20–50 years), which matches the patient’s age.
- Typically occurs near the epiphyseal ends of long bones but can also be found in the pelvis. The acetabulum is a less common site.
- Characteristic imaging appearances include well-defined osteolytic lesions adjacent to the articular surface, generally without calcification or intraosseous formation.
2. Aneurysmal Bone Cyst (ABC):
- Usually seen in individuals under 20 and in younger patients, although cases in middle-aged adults have been reported.
- Imaging often shows a septated, expansile osteolytic lesion; MRI can reveal pronounced fluid-fluid levels.
- If there is limited enhancing solid component, a pure ABC is more likely, but a large solid component lowers this possibility.
3. Metastatic Lesions, Osteosarcoma, or Other Malignant Bone Tumors:
- In older patients, bone metastases (e.g., from breast or lung cancer) should be considered. However, more extensive bone destruction or reactive sclerosis is often observed.
- Primary malignant bone tumors such as osteosarcoma may present with a soft tissue mass, widespread cortical destruction, and periosteal reaction.
Considering the imaging and clinical features in this case, a giant cell tumor of bone (GCTB) is the most likely.
III. Final Diagnosis
Based on the patient’s age (55), the presence of a lytic lesion in the left acetabulum, lesion morphology, and the findings on contrast-enhanced MRI, the most probable diagnosis is: Giant Cell Tumor of Bone (GCTB).
If uncertainties remain, a biopsy is recommended to confirm the pathological diagnosis and rule out other malignancies.
IV. Treatment Plan and Rehabilitation
Treatment Plan:
- Surgical Intervention: For resectable GCTB, the first choice is curettage with subsequent bone cement (PMMA) filling or bone grafting. If there is notable soft tissue extension or extensive local invasion, a more comprehensive surgical approach may be necessary following detailed evaluation.
- Medication: Denosumab can be effective in inhibiting RANKL and may be considered in certain cases, particularly if surgery is not feasible or in cases of postoperative recurrence.
- Radiotherapy: Generally not the first choice, but it may be considered for inoperable or recurrent lesions.
Rehabilitation and Exercise Prescription:
Postoperative rehabilitation should follow a gradual progression (FITT-VP principle) and be individualized:
- Early Rehabilitation:
- In the early postoperative period (about 1–2 weeks), protective weight-bearing is emphasized. Short-distance walking can begin with assistive devices such as braces or walkers.
- Avoid overloading and high-impact activities to prevent fracture or loosening of implants.
- Engage in range-of-motion exercises for the hip joint (passive or active) to maintain joint flexibility.
- Mid-phase Training (approximately 2–6 weeks):
- Gradually increase weight-bearing. Perform light strength training daily, such as straight-leg raises and isometric/ isotonic exercises for hip muscles.
- If tolerated, introduce aquatic exercises (swimming or water walking) to reduce stress on the hip while building muscle strength.
- Late-phase Training (6 weeks and beyond):
- After bone healing or when repair is stable, moderate weight-bearing activities can be introduced, such as weight-bearing walks or aerobic workouts (e.g., elliptical or stationary cycling).
- Ensure adequate nutrition and sufficient intake of calcium and vitamin D to aid bone recovery.
If the patient presents with fragile bones or other comorbidities, training intensity and pace should be adjusted under guidance from specialists and rehabilitation therapists. Regular monitoring of bone healing and soft tissue status is recommended to assess risks in a timely manner.
Disclaimer:
This report is based solely on the provided imaging and brief clinical information, serving as a reference for analysis. It cannot replace in-person consultations or professional medical advice. Final diagnosis and treatment should be determined by integrating the patient’s complete medical history, pathological examination, and specialty assessments.
Human Doctor Final Diagnosis
Pelvic bone giant cell tumour