Upper limb AVF with combined soft tissue and osseous involvement



Clinical History
14-year-old female with congenital swelling of the right upper limb, progressive over time, was operated twice in other institutions with no previous available records.
Imaging Findings
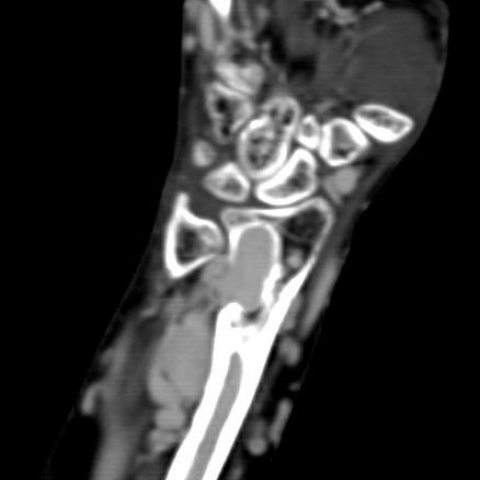
CT Angiography revealed extensive vascular malformation of the right upper limb with a dilated serpentine network of arteries and veins, multiple sites of anomalous communication, the largest at the level of the brachial artery and vein, with manifest dilated subclavian artery and vein. There was also involvement of the intraosseous vessels, with hugely prominent nutrient artery grooves at the metaphysis of multiple bones with extensive vascularization of the whole medullary spaces being filled by aneurysmally prominent arteries enhancing in similar pattern to the extraosseous vessels with subsequent bone deformity and cortical erosions. Conventional angiography showed similar findings with blush enhancement of the medullary spaces. Additional MRI revealed vascularization of medullary spaces with signal void changes and significant dilated left and right heart ventricles with high cardiac output of 12 liter per minute in this child, weighing 45 kg, reflecting risk of heart failure.
Discussion
Vascular malformations of the limbs are rare congenital anomalies with only 20% of these cases reported to have associated osseous involvement [1]. According to the international society for the study of vascular anomalies (ISSVA), vascular anomalies are divided into vascular tumours and vascular malformations (VM). Vascular tumours are further subdivided into benign, borderline and malignant tumours, while VM are further classified into 5 types: the 1st is the simple type (one type of malformation in the lesion as capillary or venous or lymphatic or arterial), AVM and AVF are also included in this group, the 2nd type of VM is the combined type (two or more malformations in the same lesion as CVM, CAVM, CLAVM), the 3rd type of VM are malformations of major named vessels, also called truncal malformations, and these are further classified according to the type of the involved vessels (lymphatics, veins, arteries ) or classified according to the nature of the defect as abnormalities of origin, course, length, diameter, related valves etc. The 4th type of (VM) includes those malformations associated with other anomalies such as VM with limb growth anomalies (Parkes Weber syndrome, Klippel Trenaunay syndrome ), VM with lipomatous hypertrophy (CLOVES syndrome, Bannayan RileyRuvalcaba sd ), VM with brain anomalies (Macrocephaly, Microcephaly, Sturge-Weber syndrome) and VM with osseous lesions (Maffucci syndrome). The 5th group includes the provisionally unclassified lesions similar to verrucous hemangioma, angiokeratoma, and angiomatosis of soft tissues [2, 3].
Our case, in spite of the extensive appearance, could possibly present a case of simple high flow AVF. This consideration is basically due to the extensive shunting related changes. The osseous involvement appears to be secondary to the VM rather than being a primary element of the malformation. It may also present a combined high flow VM such as CAVM, which may require histopathological correlation. In our case there were no observed limb growth anomalies or lipomatous hypertrophy which are seen in the 4th type of VM. There were also no associated skin lesions or adipose tissue proliferation which are found in unclassified conditions as angiokeratosis and angiomatosis of the soft tissues [4].
This case demonstrates the excellent depiction of the osseous involvement by CT while MRI further confirms the findings and reveals the effects of shunting over the heart with an extensive rise of cardiac output.
Differential Diagnosis List
Final Diagnosis
Upper limb AVF with soft-tissue and osseous involvement
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
CT Angiography






MRI CARDIAC



Conventional Angiography


Medical Imaging Analysis Report
1. Imaging Findings
The patient is a 14-year-old female with congenital swelling of the right upper limb who has undergone multiple surgeries. The currently provided CT, MRI, and angiography imaging data show:
- Extensive vascular anomalies are observed in the right upper limb, manifested as tortuous, dilated vascular appearances, indicating the presence of a high-flow arteriovenous shunt (AVF) or a combined-type vascular malformation (e.g., CAVM).
- Bone changes: The cortical structure around the shoulder joint and in the humerus exhibits alterations such as bone deformity or thickening related to the vascular malformation, presumably caused by prolonged high-flow vascular shunting.
- In the soft tissues, abundant vascular channels can be seen, which show significant enhancement after contrast, suggesting prominent arteriovenous flow pathways.
- An MRI-based cardiac function evaluation shows an increased cardiac output (CO = 12.2 L/min), indicating elevated cardiac load due to high-flow shunting in the systemic circulation.
- At present, there is no obvious limb length discrepancy, skin thickening, or excessive fat deposition, and no significant skin surface lesions are observed.
2. Potential Diagnoses
Based on the patient's age, history of congenital vascular malformation, and imaging findings, the following diagnostic or differential diagnoses can be considered:
- High-flow arteriovenous fistula (AVF): A simple type of high-flow vascular malformation in which an artery is directly connected to a vein. It often leads to local vascular structural disruption and distal venous return compromise, consistent with the extensive arteriovenous shunting seen on imaging.
- Combined-type high-flow vascular malformation (CAVM): A vascular malformation composed of arteries, veins, and other vascular elements, potentially resulting in more complex hemodynamics and tissue changes. Clinical and imaging findings are in line with this case, but pathological or dedicated imaging analyses are required for confirmation.
- Other vascular malformations with bony involvement: Such as Parkes Weber syndrome or Klippel-Trenaunay syndrome. However, there is currently no clear evidence of limb hypertrophy, skin changes, or superficial vascular tumor-like lesions, so these possibilities are relatively low.
3. Final Diagnosis
Considering the history of congenital right upper limb swelling progression, multiple surgeries, and current imaging features (high-flow vascular shunt, bone changes, elevated cardiac output, etc.), the most likely diagnosis is:
High-flow arteriovenous fistula (AVF) or combined-type high-flow vascular malformation (CAVM). Further pathological or specialized examinations are needed to confirm the specific type.
4. Treatment Plan and Rehabilitation
4.1 Treatment Strategy
- Interventional therapy: For high-flow arteriovenous fistulas or combined-type vascular malformations, endovascular embolization with coils or other embolic agents is commonly used to block abnormal shunting pathways, thereby reducing the high-flow load on the heart and alleviating local symptoms.
- Surgical treatment: If interventional measures fail to achieve adequate control, or if local tissue destruction and severe functional impairment occur, surgical ligation or partial resection of the malformed vessels may be considered. A thorough assessment of possible bleeding risks and impact on surrounding normal structures is necessary.
- Comprehensive management: Multidisciplinary collaboration with vascular surgery, orthopedics, cardiology, and other specialties is often required to manage complications (such as excessive cardiac load) and to monitor for postoperative recurrence or new shunts.
4.2 Rehabilitation / Exercise Prescription Recommendations
Because vascular malformations can lead to fragile local vessels and increased cardiac load, rehabilitation should focus on controlling exercise intensity and preventing trauma. The FITT-VP principles (Frequency, Intensity, Time, Type, Progression, Volume) can be referenced as follows:
- Type: Primarily choose low-impact forms of aerobic exercise, such as light walking, seated stretching, or swimming, and avoid high-impact or weight-bearing activities that may increase local vascular pressure.
- Frequency: Start with about 3 sessions per week, gradually increasing to 4-5 times per week according to the patient's tolerance.
- Intensity: Maintain low-to-moderate heart rate zones (e.g., 40%-60% of maximum heart rate), closely monitoring heart rate and blood pressure to avoid excessive cardiac load from the high-flow shunt.
- Time: Begin with 10-15 minutes per session and gradually extend to 30 minutes, progressing slowly to avoid fatigue-related injuries.
- Progression: Adjust training load every 2-4 weeks based on patient tolerance and follow-up metrics (cardiac function, local vascular condition).
- Volume: Keep the total exercise volume moderate. If there is any sign of chest tightness, palpitations, or significant limb pain, training should be paused and medical evaluation should be sought promptly.
Throughout the rehabilitation process, pay particular attention to protecting the affected limb. Avoid trauma or excessive force that might cause bleeding or further expansion of the vascular malformation. If pain or local swelling significantly worsens, stop immediately and reassess.
Disclaimer: This report is based solely on the current imaging and clinical data. The suggested plan is for reference only and cannot replace in-person consultations or professional medical advice. For specific diagnosis and treatment, please consult the appropriate specialist.
Human Doctor Final Diagnosis
Upper limb AVF with soft-tissue and osseous involvement