


The patient was complaining of soft swellings on the dorsum of the left foot and toes, extending into the web spaces as well as to the back of the left leg. These swellings appeared over a period of 1 year and were slowly progressive.
* Multiple lobulated soft tissue masses on the dorsum of the foot, between and ventral to the lateral 3 toes, within the proximal aspect of the plantar fascia and on the back of the lower calf. Their sizes ranged from 7 x 7 mm to 3.2 x 3 x 3.2 cm.
* On plain X-ray, there were multiple rounded calcifications within their substance. Underlying bones were normal.
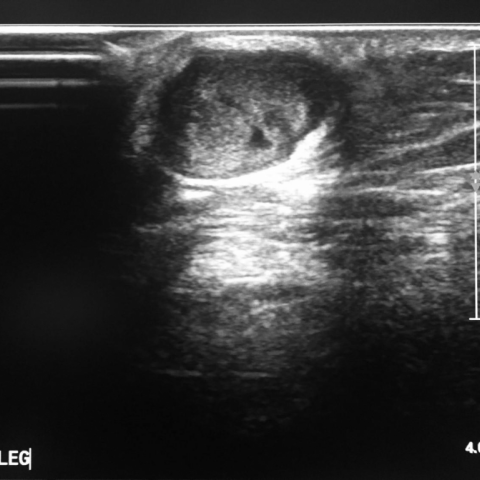
* Ultrasound revealed soft tissue masses with necrotic centre and floating echoes and intense vascularity within the solid tissue.
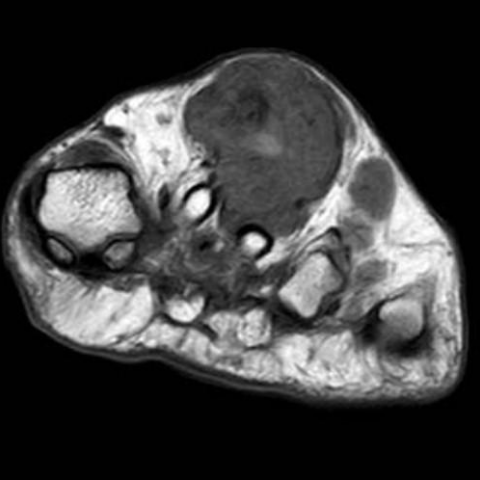
* On MRI, they appear hypointense on T1W and hyperintense on T2W and fat suppressed sequences with a hypointense rim. The largest lesion revealed central mild hyperintensity on T1W and signal void on T2W and gradient sequences, suggesting a paramagnetic effect. Other smaller foci appear hypointense on all pulse sequences (suggesting calcific foci).
* No definite abnormal marrow signal.
* No other abnormality noted.
Kaposi sarcoma (KS) is a low to intermediate grade tumor that probably originates from lymphovascular elements. The tumour has been associated with Human Herpes Virus 8 (HHV 8) and is commonly noted in patients with immune suppression, e.g. AIDS and post-transplantation.
There are 4 variants of the disease, all of which have the same histological picture. These are:
1. Classic type: characteristically forms multiple purple skin plaques that may ulcerate. They are predominantly noted in the lower limbs and rarely involve the visceral organs.
2. Endemic type: Also called lymphadenopathic, due to the presence of enlarged draining lymph nodes. This form is common in Africa.
3. Iatrogenic: This is basically related to the immunosuppression state that accompanies organ transplantation.
4. AIDS related: Kaposi sarcoma develops if the CD4 count drops to below < 200 cells/ mm3 and is considered an AIDS-defining illness. The latter two types are much more common than the first two. [1]
The most common form of the tumour is known to involve the skin. However, it can also involve the pulmonary, gastrointestinal and musculoskeletal systems. In some reports, the ureteric KS was also described.
Most studies describe the radiological features of KS in the pulmonary and musculoskeletal systems. Musculoskeletal involvement by Kaposi sarcoma is not common and usually associates skin disease by direct spread from the skin lesions. KS presents as osteolytic lesions that enhance intensely after IV contrast injection. However, the differentiation of these lesions from Bacillary angiomatosis requires biopsy. [2]
Not many reports describe the radiological appearance of cutaneous KS, partly because most lesions are plaque-like that are evaluated by the dermatologist, without any radiological evaluation. In this patient, the skin lesions were lobulated and mass-like, which required radiological evaluation prior to the biopsy. The provisional diagnosis suggested by the combined dermatological evaluation and imaging features was a fungal infection. However, biopsy revealed a Kaposi sarcoma. One research described similar MRI features, but in a patient with pulmonary KS lesions. [3] Our patient was then lost to follow-up after being informed about the biopsy result and the need to have an HIV test done.
Cutaneous and ligamentous Kaposi sarcoma, probably related to AIDS.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
















Based on the provided X-ray, ultrasound, and MRI images, the following major characteristics can be observed:
Considering the patient’s clinical symptoms (slow progression, soft tissue swelling in the foot and lower leg) and imaging findings (multiple vascular-rich, mass-like soft tissue lesions), the main differential diagnoses include:
As this patient’s biopsy has confirmed the lesion to be Kaposi’s Sarcoma, and in light of the clinical presentation and typical imaging features (multiple lobulated soft tissue lesions, abundant blood flow, significant enhancement), the most likely final diagnosis is:
Kaposi’s Sarcoma.
If further clarification of the extent of the lesions or overall systemic evaluation is needed, relevant laboratory tests (including HIV testing, immune function assessment, etc.) and imaging studies of other regions are recommended.
Based on the characteristics of Kaposi’s Sarcoma and the potential associated immunologic status, the following treatment strategies can be considered:
Since the lesions mainly involve the foot and lower leg soft tissues, it is important to balance maintaining stability in the affected area with performing functional exercises. Prolonged inactivity could lead to decreased muscle strength or limited joint mobility. Below is a stepwise, individualized example:
Throughout the rehabilitation process, warming up before exercise and proper cool-down afterward should be emphasized. High-impact or intense jumping exercises should be avoided. If there are concerns like bone fragility, improper footwear, or restricted joint mobility, adjustments should be made under the guidance of a rehabilitation or sports medicine specialist.
This report is based solely on the provided medical history and imaging data for reference purposes and does not substitute for an in-person consultation or professional medical advice. If you have any questions or if your condition changes, please seek medical attention promptly and follow the guidance of a specialist.
Cutaneous and ligamentous Kaposi sarcoma, probably related to AIDS.