Scoliosis secondary to spinal osteoblastoma


Clinical History
A 21-year-old man came to our outpatient clinic with progressive scoliosis and back pain that did not improve with the intake of non-steroidal anti inflammatory drugs (NSAID).
Imaging Findings
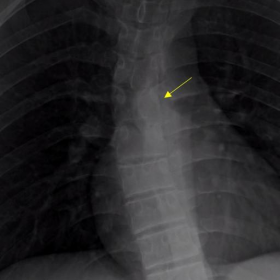
Plain film showed short thoracic dextroscoliosis with a doubtful sclerotic lesion on the left side of T6. Old films (3 years ago) showed that the scoliosis was already present without sclerosis (Fig. 1).
MRI showed an expansile bone lesion located in the lamina and left facet of T6 with a low signal intensity in T1WI and T2WI. Contrast-enhanced FS T1WI demonstrated heterogeneous enhancement of the lesion with an arterial and early dynamic enhancement type 1 curve (Fig. 2 and 3). The lesion was surrounded by marked oedema of the vertebral bodies and posterior elements of T5, T6 and T7, extending to neural foramenes, para-spinal muscles and posterior left ribs. Facing the findings, a complementary CT scan was performed confirming an expansile bone lesion with a mineralised bone matrix associated with enlargement and sclerosis of the posterior ribs, spinous process, interspinous ligament calcification and secondary dorsal kyphosis. (Fig. 4).
Discussion
Plain films are the initial method of choice for the evaluation of scoliosis. Atypical scoliosis need further imaging procedures to rule out secondary causes of scoliosis. Indications for MR imaging in a patient with scoliosis are: age <10 years, back pain, unusual curve pattern, rapid curve progression, neurological deficiency, neck stiffness and headache [1]. In our patient, MR imaging was obtained because of progressive painful scoliosis and short curve. Once the bone lesion was identified in MR imaging, a CT scan was performed to characterise the lesion, to assess the extent of osseous involvement and the degree of cancellous and cortical bone loss.
The slow evolution of the lesion, at least 3 years, with sclerosis, bone remodelling together with the absence of soft tissue mass or personal history of cancer made malignancies such as osteoblastic metastases and osteosarcoma unlikely. In the posterior spinal elements without aggressive appearance differential diagnosis should include: chondroblastoma, osteoid osteoma and osteoblastoma [2]. The lesion didn’t show chondral matrix, therefore chondroblastoma was less likely. Taking into account the clinical context, imaging characteristics and size of the lesion, the diagnosis of osteoblastoma was suggested and confirmed later by biopsy.
Osteoblastoma is a solitary, benign bone-forming tumour that occurs in the spine and long bones of young adults. Although the histological characteristics are similar to osteoma, the findings in imaging and clinical behaviour are different. Unlike osteoid osteoma, osteoblastoma is larger than 2 cm in size and patients complain of dull pain that does not worsen at night and does not improve with the intake of NSAID.
In CT spinal osteoblastoma shows an expansile lesion in posterior elements with a mineralised bone matrix and narrow transition zone. MRI features tend to be non-specific and often overestimates the lesion size due to the inflammatory response involving several adjacent bones and the surrounding soft tissues (called the "flare phenomenon”). Depending on the level of matrix mineralisation the signal intensity pattern changes, from a low to isointense signal intensity on T1Wi and from a low to high signal intensity on T2Wi. Intense contrast enhancement with gadolinium is noted given the vascular nature of the tumour. Osteoblastomas can show a type 1 curve of dynamic enhancement, manifested with an early onset of enhancement, a rapid and linear progression of signal intensity and a subsequent gadolinium washout. However, this type of curve is not specific to differentiate between benign and malignant bone tumours. Usually a biopsy is performed to confirm the diagnosis. [2, 3, 4, 5].
Differential Diagnosis List
Final Diagnosis
Spinal osteoblastoma
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Scoliosis secondary to spinal osteoblastoma


Scoliosis secondary to spinal osteoblastoma


Scoliosis secondary to spinal osteoblastoma




Scoliosis secondary to spinal osteoblastoma



Medical Imaging Analysis Report
1. Radiological Findings
Based on the provided X-ray, CT, and MRI images, a lesion exhibiting partially expansive characteristics along with both bone sclerosis and destruction is observed in the thoracolumbar spine (primarily in the posterior elements such as the pedicle and lamina). The specific radiological features are as follows:
- X-ray Plain Film: A mild scoliosis is noted in the thoracic region. The posterior part of the vertebral body shows a somewhat coarse texture with uneven density, and the lesion appears sclerotic with localized bone changes.
- CT Scan: In the lesion area of the pedicle or lamina, a clear boundary of bone proliferation and destruction is visible, with mild expansion. Spotted or nodular calcifications are seen internally, and the margin shows apparent sclerosis without a significant soft tissue mass.
- MRI Findings: On T1-weighted images, the lesion appears isointense or slightly hypointense, while on T2-weighted images, the signal varies (depending on the degree of calcification or ossification). Surrounding edema or inflammatory signals (“flare phenomenon”) are observed. The lesion demonstrates significant enhancement on contrast imaging, indicating a relatively rich blood supply.
Overall, the lesion shows relatively slow growth with no obvious malignant features and no extensive soft tissue tumor formation, consistent with the imaging characteristics of a benign bone tumor.
2. Potential Diagnosis
Based on the patient’s age, clinical symptoms (progressive scoliosis, back pain not significantly relieved by NSAIDs), and imaging findings indicating a focal benign lesion in the posterior part of the vertebral body, the following possibilities are considered:
- Osteoid Osteoma
Common in adolescents, typically presents with severe nocturnal pain that responds well to NSAIDs, and usually measures <2 cm. In this case, the patient’s pain does not worsen at night, and the lesion is larger; thus, it is less likely. - Osteoblastoma
Often occurs in adolescents and young adults, frequently found in the posterior elements of the spine, with lesions larger than 2 cm. Patients often have persistent dull pain not significantly relieved by NSAIDs. Both the imaging findings and clinical presentation in this case strongly support this diagnosis. - Chondroblastoma
Usually occurs in the epiphysis or apophyseal region and can involve the posterior spine. However, on imaging, cartilage matrix (ring-like or stippled calcifications) is often seen, which does not fully match this case. - Malignant Bone Tumors (e.g., Osteosarcoma or Metastases)
These usually progress rapidly with the presence of soft tissue masses or marked bone erosion. The lack of obvious malignant features and rapid progression in this case reduces the likelihood of malignancy.
3. Final Diagnosis
Considering the patient’s age (21 years), symptoms (continuous back pain not significantly relieved by NSAIDs), imaging findings (expansive lesion in the posterior vertebral elements, diameter >2 cm, significant enhancement, no extensive soft tissue invasion), and subsequent biopsy results, the most probable diagnosis is:
Osteoblastoma.
If any doubts remain, further confirmation through pathological examination or additional laboratory tests may be needed.
4. Treatment Plan and Rehabilitation Program
Treatment Strategy:
- Surgical Treatment: For osteoblastomas that are large, symptomatic, involve critical structures, or carry higher risk, surgical resection is the main option. Under microscopic or C-arm guidance, the lesion can be curetted or resected, followed by necessary spinal stabilization and reconstruction.
- Conservative Treatment: If the lesion is small and symptoms are mild, close follow-up and analgesics can be tried. However, in this case, with progressive scoliosis and notable pain, surgery is usually preferred.
- Other Interventions: If indicated, minimally invasive treatments such as radiofrequency ablation (RFA) may be considered. However, caution is essential, especially around the spinal cord and nerve structures, and requires expert evaluation.
Rehabilitation/Exercise Prescription Suggestions (FITT-VP Principle):
- Initial Phase (Postoperative or Acute Phase):
• Frequency: Perform short, multiple sessions of simple rehabilitation and mild stretching daily to progressively restore stability.
• Intensity: Low intensity; avoid excessive spinal load. Use bracing or professional guidance if necessary.
• Time: 5-10 minutes per session, 2-3 times a day.
• Type: Basic breathing exercises, lower limb joint activities, and mild trunk stabilization exercises.
• Progression: Over 2-4 weeks, gradually increase exercise duration and range of motion depending on incision healing and pain tolerance. - Strengthening Phase (Subacute to Recovery Phase):
• Frequency: 3-4 times per week.
• Intensity: Moderate, without inducing significant pain or fatigue.
• Time: 15-30 minutes per session, with intermittent rest.
• Type: Under professional supervision, perform core muscle strengthening (e.g., small-range planks, pelvic control exercises, swimming posture drills) and aerobic training (e.g., stationary cycling).
• Progression: Gradually increase training load and exercise difficulty based on tolerance, emphasizing correct posture and spinal neutrality. - Consolidation Phase (Long-Term Maintenance):
• Frequency: About 3 times a week, consistently.
• Intensity: Maintain moderate aerobic activity and resistance training intensity; avoid high-impact and torsional movements.
• Time: 30 minutes or more per session with a comprehensive program.
• Type: Balance exercises, yoga, Pilates, etc., to enhance core stability, improve posture, and increase flexibility.
• Progression: If needed, gradually advance to light strength training but only under medical or rehabilitation specialists’ guidance to prevent recurrence or complications from excessive stress.
Throughout rehabilitation, regularly monitor spinal stability, lesion healing, and neurological function. If severe or worsening pain or neurological symptoms occur, seek medical attention promptly.
5. Disclaimer
This report provides a reference analysis based on existing imaging data and clinical information and does not replace in-person consultation or professional medical advice. Patients should rely on individualized evaluations and guidance from orthopedic, sports medicine, or rehabilitation physicians for further treatment and rehabilitation.
Human Doctor Final Diagnosis
Spinal osteoblastoma