Intraosseous air bubbles, a sign of emphysematous osteomyelitis.



Clinical History
A 69-year man came to the Emergency Department with low back pain that irradiated to his left leg. On examination, he was febrile, tachycardic, and hypotensive. His white blood count showed sepsis. There was no significant past medical history.
An abdominopelvic-CT was performed before being transferred to the Intensive Care Unit (ICU).
Imaging Findings
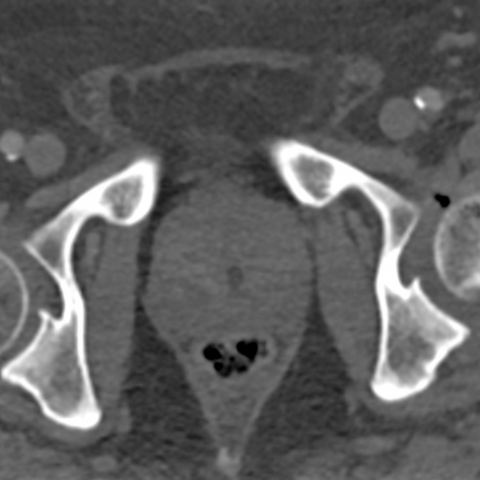
Emergency CT revealed multiple pockets of gas within the medullary cavity of the head, neck, and trochanteric region of the left femur, in addition to joint effusion accompanied by gas within the ipsilateral hip joint cavity. No cortical bone destruction was observed. (Figures 1A-1B). These imaging findings were consistent with emphysematous osteomyelitis and septic arthritis.
Thrombophlebitis of the inferior mesenteric vein was also observed in this study. (Figure 1c)
Blood cultures demonstrated Escherichia coli, and intravenous antibiotic therapy was given to the patient. Based on patient clinical deterioration, an additional pelvic and lower limbs CT was performed four days later. It showed more bubble gas within the femur and extended to the ilium, ischium and, acetabulum in the left hemipelvis. Air bubbles were also noted in the surrounding soft tissues (adductor and quadricipital compartment). (Figures 2a-2b-2c).
A magnetic resonance imaging (MRI) confirmed the progression of emphysematous osteomyelitis with necrotizing fasciitis and myositis. (Figure 3)
The patient was urgently planned for surgery. (Figures 4a-b)
Discussion
Intraosseous gas was first described as a sign of osteomyelitis by Ram in 1981 [1]. Emphysematous osteomyelitis (EO) is a rare, aggressive, and potentially fatal variant of osteomyelitis related to gas-forming organisms and usually secondary to hematogenous spread [2,3].
EO is usually a clinically unsuspected condition that is diagnosed upon radiological findings. It most commonly affects patients with significant underlying comorbidity (malignancy, DM, alcohol abuse, etc). It is related to high mortality, requiring early diagnosis and aggressive therapeutic intervention [2,3].
In our case, the source was suspected to be acute diverticulitis which complicated inferior mesenteric vein thrombophlebitis. Escherichia coli was found in blood, as well as in articular and bone cultures. Surprisingly, our patient has not known comorbidities.
Computed tomography (CT) constitutes the imaging modality of choice because it is the most sensitive method for detecting intraosseous gas. Typically, EO is seen as multiple (more than 3) irregular small foci of intramedullary gas, without associated cortical destruction. This pattern was named as “pumice stone” sign. (4) Accompanying soft tissue emphysema is also identified in the majority of EO cases and MRI is the modality of election for this compromise. MRI is essential to detect soft tissue collections that could be aspirated to reach the diagnosis and to obtain the isolation of microorganisms involved in the infection.
Diagnosis of septic arthritis was given by the presence of gas within the joint cavity, as this is a specific sign of septic origin (while joint effusion alone can be observed in many other conditions).
A key imaging feature of EO is the lack of associated cortical bone destruction: the combination of both intraosseous and extraosseous gas without cortical destruction is very specific to this entity [4].
The most common sites of EO, include the pelvic bones (38%), vertebral bodies (32%), and femurs (24%) [4].
Alternative considerations resulting in intraosseous gas include trauma, postsurgical change, lymphangiomatosis of the bone, degenerative disease, osteonecrosis, and neoplasm [5].
In the absence of a history of surgery, trauma, or degenerative change, the intraosseous gas in the appendicular skeleton is highly suggestive of emphysematous osteomyelitis. However, the intraosseous gas in vertebral bodies is generally due to a non-infectious cause, most commonly being a degenerative process.
Treatment of patients with EO should be aggressive with long term (at least 4 weeks) antibiotic therapy in addition to surgical debridement [5,6].
Our patient was attended to in the ICU for 41 days and surgical debridement was needed several times, including Girdlestone resection arthroplasty. Patient evolution was satisfactory being discharged after completing the full course of antibiotics.
Differential Diagnosis List
Final Diagnosis
Emphysematous osteomyelitis due to Escherichia coli
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Contrast-enhanced abdominopelvic CT performed in emergency. Axial images


Pelvic CT performed 4 days later. Axial and coronal bone windowing images; axial soft tissues windowing image



Pelvic MRI. Axial gadolinium-T1 and PD-SPAIR weighted images


Photographs taken in the operating room


Radiological Findings
Based on the patient’s provided CT and MRI imaging of the abdomen and pelvis, the following key features were observed:
- Multiple small gas density shadows can be seen in both acetabula and the proximal femurs (with a “spongy” or “porous” pattern), suggesting the presence of intraosseous gas.
- Free gas within the joint cavity can also be observed, especially more noticeably in the left hip joint, consistent with the “intra-articular gas” sign.
- Local gas within the surrounding soft tissues (including muscle and fascial planes), indicating soft tissue gas involvement.
- No obvious large-scale cortical destruction on CT, but localized decreased bone density and blurring can be seen, suggesting inflammatory changes.
- MRI sequences show short T1 and long T2 signals in affected bone marrow areas, with possible enhancement and edema in surrounding soft tissue.
- In combination with clinical findings (fever, localized pain, hematological indicators of infection), the presence of intraosseous, soft tissue, and intra-articular gas strongly suggests an infectious etiology.
Potential Diagnoses
Considering the patient’s age (69 years), acute onset of low back pain, systemic infectious symptoms (fever, hypotension, elevated white blood cell count), and the radiological findings, the primary differential diagnoses include:
- Emphysematous Osteomyelitis
Cause: Often caused by gas-producing bacteria such as Escherichia coli. Clinically, gas can be seen in the bone and soft tissues, frequently accompanied by sepsis. If the bone destruction is not prominent, a high suspicion for this disease is warranted. - Pyogenic Osteomyelitis
Cause: Bacterial infection leads to osteomyelitis. However, the presence of obvious gas within the bone is less common on CT. If gas is present, it tends to be more limited in scope. - Other Causes of Intraosseous or Intra-articular Gas
- Residual gas due to trauma or postoperative status: Not applicable here, as this patient does not have a history of major trauma or surgery.
- Degenerative changes in the intervertebral discs or joints (vacuum phenomenon): Commonly seen in spinal degeneration but rarely leads to pronounced infection or systemic symptoms.
Final Diagnosis
Taking into account the patient’s age, acute onset, severe signs of infection (sepsis), positive blood culture and bone/joint fluid culture for Escherichia coli, and imaging showing multiple foci of gas in bone, joint, and soft tissues without extensive cortical destruction, the most likely diagnosis is:
Emphysematous Osteomyelitis with Concomitant Septic Arthritis
This conclusion is primarily based on the following:
- Gas-producing bacteria (E. coli) isolated from blood, bone, and joint fluid cultures, confirming the pathogen.
- Multiple irregular intraosseous gas pockets (“spongy” or “porous” appearance) along with soft tissue and intra-articular gas are classic radiological manifestations of emphysematous osteomyelitis and septic arthritis.
- Lack of clear traumatic or surgical history supports an infectious etiology of gas production.
Treatment and Rehabilitation Plan
Based on the final diagnosis, the treatment goals are to control the infection, prevent further damage to bone and joints, and improve functional status. Main measures include:
- Antimicrobial Therapy
- Administer broad-spectrum intravenous antibiotics targeting gas-producing bacteria (such as E. coli) for at least 4 weeks or longer, adjusting according to inflammatory markers and clinical response.
- Closely monitor inflammatory indicators (e.g., C-reactive protein, white blood cell count) and clinical symptoms. Adjust antibiotics regimen as needed based on culture results or antibiotic sensitivity tests.
- Surgical Intervention
- For significant abscess or severe bone destruction, debridement or partial resection of the affected joint (e.g., Girdlestone procedure) may be performed to remove the infection focus.
- After surgery, continue intensive antimicrobial therapy and enhance tissue repair with functional rehabilitation exercises.
- Supportive Care
- Provide adequate nutritional support and maintain fluid and electrolyte balance. If necessary, use intravenous fluids or vasopressors to stabilize hemodynamics.
- Manage complications such as prevention and treatment of deep vein thrombosis, and provide proper nursing to prevent pressure ulcers.
- Rehabilitation and Exercise Prescription
- Acute Phase: The patient should primarily rest in bed with immobilization of the affected limb, avoiding weight-bearing and excessive activity. Under guidance, mild passive joint movement can be performed to prevent contractures.
- Subacute Phase: Once inflammation is initially controlled, begin safe sitting and simple lower limb muscle strengthening (such as isometric quadriceps contractions). Training frequency can be 3-4 times per week, 10-15 minutes each session, maintaining an intensity that causes mild fatigue but does not exacerbate pain.
- Later Rehabilitation: As infection control and tissue healing progress, gradually increase weight-bearing on the affected limb. Walking training can begin with crutches or a walker, increasing time and distance in a stepwise fashion. Each week, 5-10 minutes of aerobic activity can be added according to tolerance. Monitor heart rate and pain level, and maintain a stable gait and breathing.
- Individualized Adjustment: For patients with osteoporosis or poor cardiopulmonary function, further reduce exercise intensity and closely monitor vital signs and bone/joint pain. Regular follow-up of bone density, liver and kidney function should be performed, and imaging re-evaluation should be done to assess rehabilitation progress.
Disclaimer
This report provides a reference analysis based on the existing medical history and imaging data and does not replace an in-person consultation or professional medical decision-making. Patients should follow the guidance of a specialist physician, adopting individualized treatment and rehabilitation plans according to their specific condition.
Human Doctor Final Diagnosis
Emphysematous osteomyelitis due to Escherichia coli