Retroscapular hydatid cyst



Clinical History
A 30-year-old woman consulting for a right retro-scapular swelling. According to the patient, this swelling has been evolving for a year without pain or fever. It is only the gradual increase in size, which pushed her to consult.
She does not have a past medical history, but it is interesting to know that she is from a rural region where she is frequently engaged in agricultural activities with the presence of sheeps and dogs in her entourage.
A preliminary ultrasound was performed showing a subcutaneous cystic mass extended from the posterior shoulder region to the supraclavicular region of the neck.
Considering the ultrasound characteristics and the large size of the mass, an MRI was performed.
Imaging Findings
Axial turbo spin-echo T2-weighted image of the shoulder, illustrated at 1,5 T with (a slice thickness of 3 mm, field of view 36 cm, matrix 512x205, TR: 4500 ms and TE: 120 ms), showed a subcutaneous mass, in the right retro-scapular area, with high signal intensity. It was well surrounded by a thick regular wall with internal thick and thin septations.
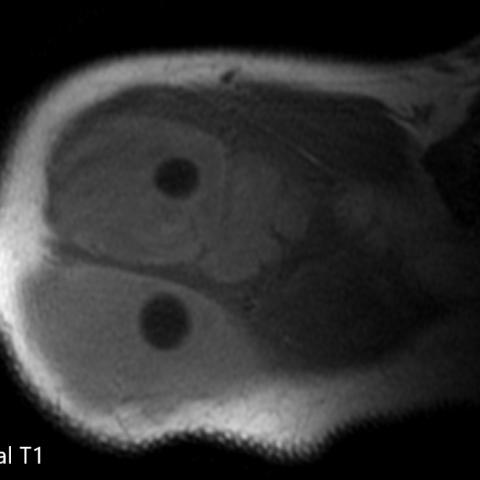
Axial T1-weighted Image showed intermediate Signal intensity of the mass.
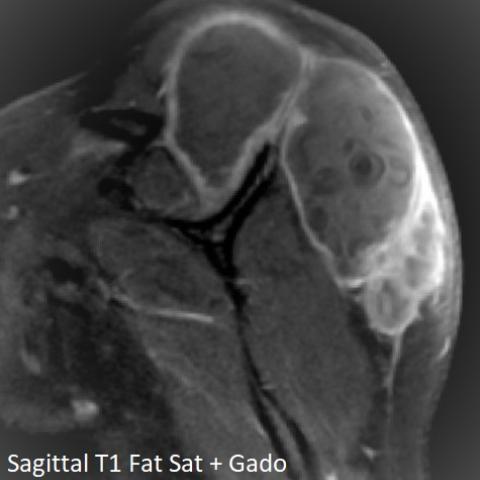
Sagittal fat-suppressed gadolinium contrast-enhanced T1-weighted image showed an intense enhancement of both of thickened walls and septations of this mass. The maximum cyst expansion was posterior, above the infraspinatus muscle, then extending in the supra-spinous fossa and compressing the supraspinatus muscle.
That cystic lesion showed round hypointense formations in its internal part in all the sequences (T1- weighted, T2- weighted, T1- weighted after Gadolinium + fat sat) a diagnosis of hydatid cyst has been made.
Given this MRI appearance, a hydatid serology was requested which came back positive for Echinococcus granulosus. So, a diagnosis of hydatid soft tissue disease has been retained.
Later, the orthopaedic surgeons performed en bloc surgical resection with albendazole injection before and after surgery. During six months of follow-up, no operative complications have occurred, and the patient was clinically well.
Discussion
Background
Hydatidosis is a parasitic disease caused by tapeworms of the genus Echinococcus. It is a benign condition that is considered endemic in many African countries [1]. Even in endemic countries, its primary localization in soft tissue is rare (between 1% and 5 % of all hydrated localizations) and it is considered an unusual event [2].
If not complicated, there are no specific symptoms apart from the soft tissue swelling. Otherwise, the possible main complications are infection, rupture or compression of neighbouring structures [3].
Ultrasonography remains a valuable first-line examination in visceral hydatidosis cases. It can detect, correctly, daughter vesicules for diagnosis and characterize the lesion according to Gharbi classification [4].
The Contrast-enhanced Computed Tomography does not offer high specificity, but it can specify the number, the size, the topography and the vascular relationships of the cyst, especially, if surgical management is decided.
In soft tissue localization, MRI is a method of choice. It is able to establish a positive, differential and topographic diagnosis. It offers a better study of the cyst wall, as well as its contents, thus, allowing the identification of certain appearance characteristics of Echinococcosis [5].
The cyst wall, representing the pericyst, appears as a hypointense signal border on all sequences, mainly on T2-weighted sequences. It can demonstrate a moderate peripheral enhancement. This enhancement is specific in hydatid disease of the musculoskeletal tissues, which is not seen in other localizations [6]. It can be intense and remarkable in case of infection, due to the intense vascularization of the pericyst and the adjacent inflammatory reaction.
In typical cases, the pathognomonic appearance is that of "cyst in the cyst" (30% of cases) is related to the presence of daughter vesicles from the proliferation of the endo-cyst or proliferous membrane. On T1-weighted sequences, these vesicles appear with a low remarkable signal compared to the surrounding liquid hydatid. On T2-weighted sequences, they appear in hypo or hyper intense signal according to the presence or not of tapeworm head. In the event of cystic involution, the proliferous membrane can detach and be the source of a linear or banded hypointense signal inside the cyst on all the sequences called "Serpent sign".
These Imaging features on MRI with the serology hydatid tests can help to confirm the positive diagnosis and can avoid an unnecessary cystic puncture to make the differential diagnosis with other neoplastic masses. The treatment should be constantly surgical with an excision of the cyst. But the total resection depends on the size, the location depth and the contact with vascular-nervous elements. It is recommended to introduce anthelmintics before surgery to reduce the risk of dissemination during the excision and after surgery to reduce the risk of recurrence postoperatively.
However, local recurrence is possible; thus, it requires close monitoring. This follow-up is ensured by regular control of the hydatid serology and the clinical examination. Thus, on the slightest suspicion, the ultrasound is effective to confirm any recurrence.
Differential Diagnosis List
Final Diagnosis
Hydatid cyst
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures
Axial T2

Axial T1
Sagittal T1 Fat Sag + Gado
Medical Analysis Report
1. Imaging Findings
Based on the provided MRI scans (including T1-weighted images, T2-weighted images, T1 fat-suppressed enhanced sequences) and ultrasound results, a large cystic lesion is observed in the area extending from the right shoulder dorsal side to the supraclavicular region of the neck:
- The lesion is located in the subcutaneous soft tissue with a cystic appearance, well-defined margins, and relatively homogeneous internal signals. However, multiple septations or “cyst-within-cyst” structures are noted.
- On T2-weighted images, the cyst wall shows low signal intensity (a low-signal band), and local enhancement is observed in the cyst wall and surrounding soft tissues.
- On T1-weighted images, part of the cyst contents appear as low signal. There may be daughter cysts or membranous structures within the cyst, exhibiting signal differences.
- The lesion extends upward into the neck, but there are no clear signs of bone destruction or severe compression of nerves or major vessels.
2. Potential Diagnoses
Given that the patient is from an endemic area (with close contact with dogs, sheep, etc.) and the imaging suggests a multi-cystic or “cyst-within-cyst” appearance, the main potential diagnoses include:
- Soft Tissue Hydatid Disease (Echinococcosis)
- Epidemiological factors: The patient has close contact with animals such as dogs and sheep, which is a risk factor for infection.
- Imaging characteristics: Typical “cyst-within-cyst” or septated lesions. On T2-weighted images, a low-signal cyst wall band can sometimes be seen, and occasionally the “snake skin” sign is indicated.
- Other Soft Tissue Cystic Lesions (e.g., large bursitis or ganglion cysts, hematoma, subcutaneous lymphangioma, etc.)
- Bursitis, ganglion cysts: Commonly found around joints or tendons, often near joint capsules. They usually present with more uniform imaging signals and generally lack “cyst-within-cyst” features.
- Hematoma: Often correlated with a history of trauma; MRI may show layering signals or signals of hemosiderin deposition.
- Subcutaneous lymphangioma: Typically shows distinct features in earlier stages, and the intralesional blood flow signal or septation pattern differ from those of hydatid disease.
3. Final Diagnosis
Considering the patient’s epidemiological history (exposure to dogs, sheep, etc.), the relatively typical imaging findings (multiple cystic structures, “cyst-within-cyst” appearance, characteristic cyst wall signals), and the common occurrence of this parasitic disease in endemic regions, the most likely diagnosis is:
Soft Tissue Hydatid Disease (Echinococcosis)
If serological tests (hydatid serology) and further pathological/surgical exploration confirm it, the diagnosis can be definitively established. If there is still doubt, additional serological and imaging examinations, or pathological confirmation from surgical specimens, can be performed.
4. Treatment Plan and Rehabilitation Strategy
Treatment Strategy:
- It is recommended to administer antiparasitic medication (e.g., albendazole) before and after surgery to reduce the risk of intraoperative parasite spread and postoperative recurrence.
- If the cyst can be completely removed surgically, an attempt at complete cyst resection should be made. For cases where the cyst is large and close to vital vessels and nerves, the surgical risks and benefits must be carefully evaluated.
- Postoperative follow-up and serological monitoring are crucial to detect potential recurrence in a timely manner.
Rehabilitation and Exercise Prescription:
- Postoperative Phase 1 (Weeks 1-2): Focus on protective movements and basic shoulder joint activities, along with local wound care. Under professional guidance, gentle active and passive movements of the shoulder joint can begin, avoiding excessive stretching pain.
- Postoperative Phase 2 (Weeks 2-6): If the incision heals well, gradually increase the range of motion (ROM) exercises for the shoulder and begin light isometric contractions to prevent muscle atrophy and joint stiffness.
- Postoperative Phase 3 (Week 6 onward): In the absence of complications, progressively increase resistance training intensity, targeting the shoulder and back muscles. Follow the FITT-VP principle (Frequency, Intensity, Time, Type, Progression, Volume), for example:
- Frequency: 2-3 times per week.
- Intensity: Start with low loads based on individual tolerance, gradually increasing.
- Time: About 30 minutes each session, ensuring no significant discomfort or fatigue.
- Type: Functional shoulder exercises combined with resistance training, such as resistance bands or light dumbbells.
- Progression: Adjust the training volume every 1-2 weeks depending on patient tolerance.
- If there is persistent local pain or additional soft tissue injuries post-surgery, individualized adjustment should be made under the guidance of a physician and rehabilitation therapist.
During rehabilitation, attention should be paid to the patient’s overall physical condition. If there is bone fragility or poor cardiopulmonary function, the exercise program should be further individualized at a slower pace, with enhanced attention to safety.
Disclaimer: This report aims to provide a reference for medical analysis and does not replace an in-person consultation or professional medical advice. Specific treatment and rehabilitation plans should be carried out under the guidance of qualified healthcare professionals.
Human Doctor Final Diagnosis
Hydatid cyst