A “bump” in popliteus tendon insertion



Clinical History
A forty-seven year old female presented with the complaints of progressive right knee pain for 6 months, aggravated by activities. On clinical examination, lateral joint line tenderness and swelling were noted. There was no history of trauma or fever.
Imaging Findings
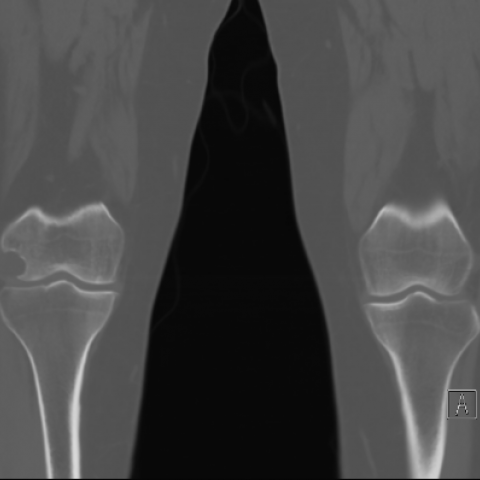
Imaging workup of the patient was performed. Knee radiograph showed notching of the lateral femoral condyle. USG showed a cystic lesion with few thin smooth septations, without any internal vascularity, abutting the lateral femoral condyle.
CT and MRI showed a well-defined lobulated, partly exophytic, smooth rim enhancing cystic lesion with few thin smooth enhancing septations, adjacent to the lateral femoral condyle at the site of popliteus tendon attachment, measuring 2.8 x 2.0 x 1.8 cm.
Small extension along the popliteus tendon sheath with mucoid degeneration of the popliteus tendon was seen. The lesion caused indentation of the adjacent soft tissues and smooth scalloping of the lateral condyle with a thin sclerotic rim. No extension to the articular surface was seen. No diffusion restriction, haemorrhage, fluid level or enhancing soft tissue component were noted within the lesion.
Discussion
Background
Ganglion cysts are benign cystic lesions that occur in collagenous structures due to mucinous degeneration produced by persistent irritation, recurrent damage and ischemia. They are filled with gelatinous fluid rich in hyaluronic acid and other mucopolysaccharides, surrounded by dense connective tissue, and lack synovial epithelial layer [1]
Ganglion cysts are classified into four types viz. intra-articular, extra-articular, intraosseous and (rare) periosteal. [2]
The common locations of ganglion cyst in the knee are: joint capsule, anterior cruciate ligament, posterior cruciate ligament, Hoffa fat pad and menisci. It may also occur in atypical locations like tendon sheaths, within muscle bundles, or adjacent to tibiofibular joints. [3] However, ganglion cyst involving the popliteus tendon is a rare occurrence. [4]
Clinical Perspective
Ganglion cyst of the popliteus tendon is an unusual cause of posterolateral knee pain.[4] The popliteus muscle offers posterolateral stability to the knee by internally rotating the tibia. It takes origin from the posterior surface of proximal medial tibia, extends via the popliteus hiatus, and inserts into the posterior horn of lateral meniscus and lateral margin of lateral femoral condyle. [5]
Imaging Perspective
On imaging, ganglion cyst appears as a well-demarcated rounded or lobulated fluid collection, often with sharply defined internal septations (“bunch of grapes” appearance). MR imaging shows high signal intensity on T2-weighted images and variable signal intensity in T1-weighted images depending on the protein content. Adjacent bone scalloping and pericystic oedema have also been demonstrated. [2] Ganglion cyst of tendon can resemble parameniscal cyst or intra-articular ganglion cyst in appearance, but it lacks the associated internal derangements of the knee which are common in the latter entities.
Outcome
Excision biopsy of the lesion was done which revealed a pearly white cyst over the popliteus tendon. Histopathological examination showed a cyst with proliferating capillaries, focal myxoid change, fibrin deposits and calcified debris, with a dense collagenous wall without lining epithelium; which was consistent with ganglion cyst.
Take-Home Message / Teaching Points
Ganglion cyst of the popliteus tendon is a rare lesion, the diagnosis of which requires a multimodality approach for differentiating from other lesions of the knee. MRI is a valuable tool for identifying typical patterns that aid in determining the accurate diagnosis, thereby guiding specific therapy and reducing unnecessary interventional procedures.
Written informed patient consent for publication has been obtained.
Differential Diagnosis List
Final Diagnosis
Mucoid degeneration of popliteus tendon with ganglion cyst
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures




I. Imaging Findings
Based on the provided X-ray, ultrasound, CT, and MRI images of the right knee joint, the following findings are noted:
- X-ray: The joint space is generally maintained. No obvious bony destruction or fracture sign is observed. There are mild degenerative changes (such as subchondral sclerosis or small osteophytes at the joint margin), with no significant abnormality overall.
- Ultrasound: A well-defined hypoechoic or anechoic, cystic structure is detected in the posterolateral aspect of the knee (near the fibular collateral ligament or popliteus tendon region). It may show septations or a “cluster of grapes” appearance, consistent with a cystic lesion.
- CT: The articular surfaces appear generally intact, and no obvious abnormal soft tissue density is found within the joint. A cystic low-density lesion with a smooth margin is noted in the region of the popliteus tendon. There is no apparent bone destruction or erosion adjacent to it.
- MRI: In the posterior aspect of the lateral tibial plateau, near the popliteus tendon, a lobulated cystic lesion is seen with high signal on T2 and low or intermediate signal on T1. The lesion has clear borders, possibly with some internal septations. Surrounding soft tissue relationships are clear, and there is no noted signal alteration in the meniscus or ligaments. The cystic lesion is adjacent to or in close contact with the popliteus tendon, suggesting a popliteus tendon-related cystic mass.
II. Potential Diagnoses
-
Popliteus tendon sheath cyst (a synovial or ganglion-type cyst of the popliteus tendon):
This type of cyst often appears as a T2 hyperintense, well-demarcated cystic lesion, commonly found within soft tissues or around tendon sheaths, and closely related to local ligaments or tendons.
-
Parameniscal cyst or intra-articular synovial cyst (e.g., collateral ligament cyst, synovial cyst):
If the lesion is near the joint capsule or associated with a meniscal tear, it could be a parameniscal cyst. However, this case shows no clear sign of meniscal injury, making this less likely.
-
Popliteal cyst (Baker’s cyst):
Usually located in the posteromedial aspect of the knee, communicating between the semimembranosus and gastrocnemius tendons. In this case, the lesion is in the posterolateral area (close to the popliteus tendon), which is atypical for a Baker’s cyst.
-
Other soft tissue mass (e.g., lipoma, synovial tumor, inflammatory lesion, etc.):
Generally, the MRI signal characteristics differ from this lesion. Also, the patient has no fever, trauma history, or systemic symptoms to suggest acute infection or malignancy.
III. Final Diagnosis
Considering the patient is a middle-aged female with chronic pain and no trauma history, along with MRI findings of a typical cystic lesion, and surgical plus pathological confirmation of a cystic structure without an epithelial lining, we conclude:
Most likely diagnosis: A tendon cyst (ganglion cyst) related to the popliteus tendon.
The pathology result also indicates that the cyst is consistent with a ganglion cyst (gel-like mucus without epithelial lining).
IV. Treatment Plan & Rehabilitation
1. Treatment Strategy
- Surgical treatment: For patients with significant symptoms, poor response to conservative management, or a large cyst affecting joint function, surgical excision (open or arthroscopic) is an option. In this case, the cyst has been surgically removed, and pathology confirmed it as a tendon cyst.
- Conservative treatment: If symptoms are mild, initial conservative care such as physical therapy, anti-inflammatory analgesics, and joint mobility exercises can be tried, with close observation of the cyst size and symptom changes.
2. Rehabilitation and Exercise Prescription
During postoperative or conservative treatment, rehabilitation exercises should be gradually intensified based on the patient’s condition. The FITT-VP principle is recommended:
- Frequency: Start with low-intensity training about 3 times per week, and gradually increase to 4-5 times per week depending on tolerance.
- Intensity: Focus on low to moderate intensity, avoiding significant pain or joint instability. Initially, non-weight-bearing or minimal weight-bearing exercises such as ankle pumps, straight leg raises, and seated knee flexion/extension are suitable.
- Time: Begin with approximately 10-15 minutes per session, progressively extending to 30 minutes, depending on patient tolerance.
- Type:
- Range of motion (ROM) exercises: Including passive knee flexion/extension and wall slides.
- Muscle strengthening: Emphasize the quadriceps, hamstrings, and calf muscles (e.g., seated or supine isometric quadriceps contractions).
- Balance and stability training: In later stages, introduce balance board exercises, single-leg stands, etc., to improve knee stability.
- Volume & Progression: Increase total training volume and intensity every 1-2 weeks as tolerated, ensuring safety and minimal pain. For example:
- Early stage: 10 minutes of low-intensity ROM exercises + 3 sets of 10 isometric quadriceps contractions.
- Intermediate stage: Add low-resistance (elastic bands or light weights) exercises for quadriceps and hamstrings, about 20 minutes each session.
- Later stage: Once joint function is sufficiently restored, consider partial weight-bearing squats, balance board exercises, etc., under professional supervision.
If significant pain, swelling, or other discomfort appears during rehabilitation, seek medical advice or consult a physiotherapist promptly.
V. Disclaimer
This report is a reference analysis based on the available imaging data and medical history. It does not replace in-person consultation or professional medical advice. In case of any uncertainties or changes in condition, please consult a specialist promptly.
Human Doctor Final Diagnosis
Mucoid degeneration of popliteus tendon with ganglion cyst