A rare case of ankle soft tissue sarcoma: 'Creeping beneath the skin'



Clinical History
A 63-year-old female patient presented with a swelling over the right ankle for 1 year, slowly growing in size. History of a surgery over the right ankle for similar complaints. No other comorbidities.
Imaging Findings
Plain anteroposterior & lateral radiograph showed an ill-defined soft tissue lesion in the posteromedial aspect of the right ankle.
Ultrasonography with colour doppler study showed an ill-defined heteroechoic lesion with significant internal vascularity.
Non-contrast computed tomography (NCCT) showed a well-defined lobulated isodense lesion measuring ~ 5.3 x 3.5 x 1.7 cm (CC X AP X TR) in the subcutaneous plane of the posteromedial aspect of the right ankle extending from the level of the distal metaphysis of tibia up to the level of tibiotalar joint approximately 3.5 cm above the Achilles tendon insertion site. There was no evidence of calcification/haemorrhage seen within the lesion. Adjacent bones appeared normal.
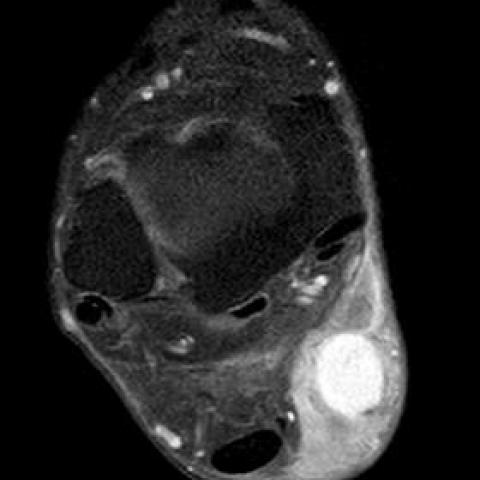
MRI (with contrast) showed the lesion to be isointense on T1WI & hyperintense on T2WI/STIR sequences. Few areas of flow voids were noted within the lesion on T2WI. The lesion showed true diffusion restriction with no evidence of gradient blooming. Surrounding subcutaneous tissue showed diffuse edematous changes. Post-contrast imaging showed significant heterogeneous enhancement within the lesion. There was no obvious infiltration into the overlying skin but infiltration of the subcutaneous fat tissue was noted.
Discussion
A. Background
Dermatofibrosarcoma protuberans (DFSP) is a rare, low-grade, locally aggressive neoplasm, accounting for approximately 6% of soft tissue sarcomas. DFSP is classified as a fibroblastic/myofibroblastic tumour. [1] Histologically, DFSP is composed of uniform spindle cells with elongated nuclei arranged in an interwoven fascicular storiform or cartwheel pattern, embedded in varying amounts of collagen. Immunohistochemically, CD34 is positive in 90% of DFSP patients. [9]
B. Clinical perspective
DFSP is more common in adults between 20 and 50 years. [1] There is no sex bias. [2] DFSP can occur in almost any part of the body, the most common site is the trunk, followed by proximal extremities; head and neck are less common.[1,2] DFSP grows slowly, ranging from several months to many years. [1] DSFP often demonstrates round, oval, or irregular soft tissue mass, and protrudes skin surfaces to different degrees. The tumour is usually solitary and relapsed cases often show lobulated or multiple nodules.
C. Imaging Perspective
On ultrasound, DFSP appears as a low echo mass with a rich blood supply. [3, 4] On CT, DFSP appears as a solitary, well-defined isodense cutaneous or subcutaneous mass, with no calcification. DFSP shows homogeneous enhancement for small tumours and nonhomogeneous enhancement for large tumours. [5–7].
On MRI, the tumour appears as a well-defined isointense mass compared with muscle on T1-weighted images and hyperintense on T2-weighted images. On contrast-enhanced T1-weighted images, the tumour demonstrates intermediate or marked homogeneous or heterogeneous enhancement. [3, 8-9] DFSP is often rich in blood supply. [4, 5]
In the report by Garg et al [5], a DFSP arising in the leg showed contiguous infiltration of the underlying bone. In another report by Thornton et al,[8] the proposed surgical margins were enlarged relying on the MR imaging findings in 2 out of 5 cases. Presurgical MRI is important for surgical plans and follow-up.
D. Outcome
The prognosis of DFSP is generally good. Surgical resection is the main treatment for DFSP. However, DFSP has a high rate of local recurrence, but little distant metastasis. [5] Postoperative follow-up is particularly important, especially in the first 3 years. [11]
E. Take-home message
DFSP is characterized by a subcutaneous well-defined soft tissue nodule or mass on plain CT/MR scans and shows intermediate-to-marked enhancement on contrast-enhanced CT/MR scans. The imaging findings for DFSP are nonspecific, but the diagnosis can be made in an appropriate clinical setting.
Differential Diagnosis List
Final Diagnosis
Dermatofibrosarcoma protuberans over the posteromedial aspect of the right ankle
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures














Medical Imaging Analysis Report
1. Radiological Findings
Based on the right ankle images provided by the patient (including X-ray, color Doppler ultrasound, CT, and MRI), the following can be observed:
- X-ray plain film: Overall, the bony structures of the ankle joint appear relatively preserved. A protruding soft tissue mass shadow can be seen with generally clear margins; no obvious osseous destruction or bone erosion is noted. The ankle joint space is largely maintained.
- Color Ultrasound: Beneath the ankle joint and surrounding subcutaneous soft tissue layer, a hypo- or mixed-echoic mass can be observed with abundant blood flow signals, suggesting rich local blood supply.
- CT Scan: In the subcutaneous region of the right ankle, there is a soft tissue density lesion with relatively well-defined margins, and its density is approximately similar to the surrounding soft tissues. Post-contrast enhancement reveals moderate to marked enhancement with local lobulation, and no obvious bone erosion is found.
- MRI: On T1-weighted imaging, the lesion’s signal is similar to that of muscle (isointense). On T2-weighted images, it appears hyperintense. Post-contrast scans show marked heterogeneous or relatively homogeneous enhancement, consistent with fibrosarcoma-like or related soft tissue tumor features. There is no significant involvement of the joint cavity. Surrounding muscles and tendons can occasionally be compressed or slightly displaced.
2. Potential Diagnoses
Taking into account the patient’s age (63), clinical presentation (a slowly growing mass in the ankle area with a previous history of local surgery), and imaging findings, the potential or differential diagnoses include:
- Dermatofibrosarcoma protuberans (DFSP): Typically presents as a slowly growing subcutaneous or soft tissue tumor. MRI often shows iso-intense signal on T1, hyperintense signal on T2, with prominent enhancement. It can have a high recurrence rate. Combined with the CD34-positive immunohistochemical results in this case, it strongly suggests the diagnosis.
- Fibrosarcoma or other fibrous soft tissue neoplasms: They can exhibit similar histological features and enhancement patterns on imaging, but usually require pathological immunohistochemistry (e.g., CD34, S-100) for differentiation.
- Synovial sarcoma and other soft tissue sarcomas: They can also present as an enhancing soft tissue mass, but are more commonly seen in younger patients, and differ in pathological markers and clinical manifestations.
- Giant pigmented nevus or other cutaneous adnexal tumors: It cannot be completely ruled out based solely on imaging; however, their imaging features typically lack a rich vascular or fibrous component, and they are more easily distinguishable histologically.
3. Final Diagnosis
Combining the patient’s clinical history (including a similar previous surgical history, slow-growing mass with local recurrence), imaging findings (subcutaneous tumorous lesion, T2 hyperintensity, significant enhancement on contrast scan), and pathological histology showing the typical storiform arrangement of spindle cells and CD34 positivity on immunohistochemistry, the most likely diagnosis is:
Dermatofibrosarcoma protuberans (DFSP).
If there are further clinical concerns, additional pathological molecular tests (such as PDGFB gene rearrangement) may be performed intraoperatively or postoperatively to confirm the diagnosis.
4. Treatment Plan and Rehabilitation Program
- Treatment Strategy:
- Surgical Resection: DFSP is characterized by locally invasive growth. Wide surgical excision (including Mohs micrographic surgery) is the first choice to reduce the risk of local recurrence. Efforts should be made to preserve ankle joint function, and preoperative MRI can be used to assess the margins if necessary.
- Radiotherapy: If the surgical margins are unclear postoperatively or if obtaining a sufficiently safe margin is not possible, adjuvant radiotherapy can be considered.
- Molecular Targeted Therapy: For inoperable or recurrent cases, tyrosine kinase inhibitors (e.g., imatinib) may be considered, particularly in situations where complete local excision or distant metastasis management is difficult.
- Rehabilitation and Exercise Prescription Recommendations:
-
Postoperative/Treatment Acute Phase (0-2 Weeks):
- Protect the affected ankle to avoid heavy loads or excessive flexion and extension.
- Light toe motion and non-weight-bearing active ankle movements can be performed to promote blood circulation.
-
Recovery Phase (2-6 Weeks):
- Gradually reduce or remove external support according to medical advice and perform ankle flexion and extension exercises.
- Use the principle of “low intensity, high repetition” initially, starting with 1-2 sets of 10-15 repetitions per set, with relatively light intensity.
-
Later Functional Training (6 Weeks to 3 Months):
- Gradually increase range of motion and muscle strength training, such as tiptoe exercises and resistance training for plantarflexion/dorsiflexion and inversion/eversion of the ankle.
- Continue with 2-3 sets per session, each set not limited to 10-15 repetitions, but proceed gradually without causing significant pain or swelling.
-
Maintenance Phase (3 Months and Beyond):
- Engage in higher-level strength and balance training, such as single-leg stands, balance board, and resistance band exercises.
- Depending on cardiovascular and skeletal conditions, low-impact aerobic exercise (e.g., cycling, swimming) may be introduced 2-3 times per week for 20-30 minutes each session.
-
Precautions:
- Because of the patient’s advanced age, pay extra attention to bone quality and cardiopulmonary function to avoid complications from excessive exercise.
- Perform appropriate ankle warming up and stretching before and after each session. If significant pain, swelling, or discomfort occurs, prompt medical consultation is advised.
Disclaimer: This report is for medical information reference only and cannot replace an in-person consultation or professional physician’s diagnosis and treatment advice. Please combine specific treatment plans and rehabilitation arrangements with actual clinical conditions and carry them out under the guidance of a professional physician.
Human Doctor Final Diagnosis
Dermatofibrosarcoma protuberans over the posteromedial aspect of the right ankle