Tuberculous spondylitis (Pott's disease)



Clinical History
A 32-year-old male patient, who was treated for pulmonary tuberculosis 17 years ago, presented with back pain, stiffness, and paraplegia developing within the last several months.
Imaging Findings
A 32-year-old male patient, who was treated for pulmonary tuberculosis 17 years ago, presented with back pain, stiffness, and paraplegia developing within the last several months. An MRI study has been performed on a 1.5 T MR scanner, with SE T1, fat-suppressed SE T1, FSE T2, post-gadolinium SE T1 weighted on three orthogonal planes. MRI study revealed that lumbar vertebrae L4 and L5, and sacral vertebra S1 and adjacent intervertebral discs were involved with a destructive process, associated with left-dominant bilateral anterior paravertebral (psoas) and epidural abscesses.
Discussion
Tuberculous spondylitis (Pott’s disease) is characterized by destruction of vertebral bodies and adjacent intervertebral disks by mycobacterium tuberculosis. The spine is the most frequent site of osseous involvement in tuberculosis, which constitutes about 1 % of patients with tuberculosis and 25-60 % of patients with osseous tuberculosis. Pott’s disease can be seen in any age group, and there is slightly increased predilection for males. The elderly, immuno-compromized patients, drug addicts, and the patients with AIDS are more affected with the disease. Clinically there is an insidious onset of back pain and stiffness, with local tenderness. Pulmonary lesions are not seen at the time of Pott’s disease in about 50 % of the patients. Mortality rate changes in between 26 to 30 %. A high degree of clinical suspicion and familiarity with the various radiologic manifestations of tuberculosis allow early diagnosis and timely initiation of appropriate therapy, thereby reducing patient morbidity. Upper lumbar and lower thoracic spine is the most frequently involved site, often with three or more contiguous vertebrae involved. L1 vertebra corpus is the most common site for Pott’s disease. An anterior predilection is seen in the vertebral body in 82 % of the cases. The disease process begins in the anterior part of the vertebral body, adjacent to either the superior or inferior end-plates. The infection spreads to involve the adjacent disk spaces by extension beneath the anterior or posterior longitudinal ligament, or by penetration of the subchondral bone plate. Involvement of the disk manifests as collapse of the intervertebral disk space. Demineralization of the end plates occurs with resorption and loss of dense margins. With progression of disease, there is development of progressive vertebral collapse with anterior wedging, leading to the characteristic angular kyphotic deformity and gibbus formation. Extension of tuberculosis from the vertebra and disk to adjoining ligaments and soft tissues is seen frequently and usually occurs anterolaterally. Subligamentous extension of a tuberculous abscess can be seen as erosive scalloping of the anterolateral surface of the vertebral bodies (called gouge defect) even distant from the primary site of involvement. Paravertebral abscesses form early and are easily seen in the thoracic region as posterior mediastinal masses. Paravertebral psoas abscess in the lumbar spine can produce significant paraspinal soft tissue opacity. The psoas abscess may even extend into the groin. Psoas abscesses may reveal amorphous or tear-drop shaped calcifications in late stages of the disease. Both computed tomography and magnetic resonance imaging are helpful in demonstrating above mentioned changes and diagnosing tuberculous spondylitis. The most important differential diagnosis is pyogenic spondylitis. Other entities that may mimic tuberculous spondylitis include vertebral body metastases, sarcoidosis, primary vertebral neoplasm (lymphoma, multiple myeloma, chordoma), and rare spinal infections such as brucellosis, fungal disease, and echinococcosis. Pyogenic spondylitis is characterized by rapid destruction, multiple abscess cavities, little new bone formation, however thickening or calcification of abscess rim and posterior element involvement are not associated. Multiple vertebral involvement which is characteristic for Pott’s disease is not observed in the case of pyogenic spondylitis. Metastases are characterized by multiple noncontiguous lesions, little soft tissue involvement, but disk destruction is not observed. Complications of Pott’s disease are angular kyphosis (called gibbus deformity), scoliosis, ankylosis, osteonecrosis, paralysis (due to spinal cord compression from epidural abscess, granulation tissue, bone fragments, or arachnoiditis). Antituberculous medical treatment and surgical interventions are the therapeutic options, depending on the stage of the disease.
Differential Diagnosis List
Final Diagnosis
Tuberculous spondylitis (Pott's disease)
Liscense
Figures
Sagittal pictures



Coronal pictures


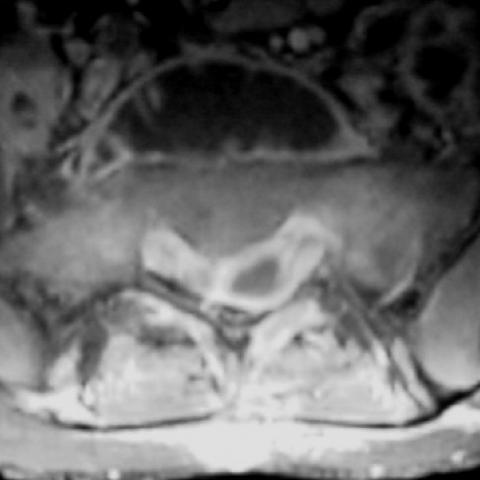
Axial images


Radiological Findings
This patient's lumbar MRI images demonstrate multiple adjacent vertebral bodies (primarily in the lower thoracic and upper lumbar segments) with bony destruction, wedge-shaped changes at the anterior margin of the vertebral bodies, and narrowed intervertebral disc spaces. Some paravertebral and posterior vertebral soft tissues show space-occupying lesions, which appear as mass-like formations or larger conglomerates. The signal suggests the possible presence of abscesses or granulation tissue. The damaged areas of the vertebral bodies are mainly located in the anterior region near the intervertebral discs. Pronounced swelling of the surrounding soft tissues is noted, and abnormal soft tissue shadows of varying extent can be observed in the paravertebral and psoas regions, possibly indicating paravertebral or psoas abscess formation. There is obvious collapse in certain vertebral bodies and a mild kyphotic deformity (increased kyphotic angle). Compared with the normal alignment of the cervicothoracic spine, a certain degree of angular curvature is seen. No extensive bony overgrowth or newly formed sclerotic margins are detected. These changes are consistent with vertebral and intervertebral disc destruction accompanied by paravertebral and paraspinal abscess formation.
Potential Diagnoses
- Tuberculous spondylitis (Pott's disease): Given the patient's previous history of pulmonary tuberculosis, the involvement of the anterior portion of the vertebral bodies and the intervertebral discs, abscess formation, slow progression, and clinical symptoms (back pain, stiffness, neurological findings), tuberculous spinal infection is highly suspicious.
- Pyogenic spondylitis: Typically progresses more rapidly, often presents with multiple abscess cavities but does not commonly involve multiple consecutive vertebrae, and usually lacks marked wedge-shaped vertebral deformities. The relatively slow progression and involvement of multiple vertebrae in this case do not fully match pyogenic spondylitis, though it still warrants differential consideration.
- Vertebral metastasis: Metastases can cause bony destruction, but usually with minimal intervertebral disc involvement. They often present as multiple, non-contiguous lesions. The imaging features in this case more strongly indicate an infectious rather than a metastatic process.
- Other rare infections (e.g., fungal or brucellar infection): Such infections can also manifest with similar vertebral and intervertebral disc destruction. However, given the patient’s history of pulmonary tuberculosis and the characteristic imaging findings, these seem less likely. Laboratory and pathogen-specific testing would be required to rule these out.
Final Diagnosis
Considering the patient's past medical history (previous pulmonary tuberculosis), imaging findings (vertebral destruction, intervertebral disc involvement, surrounding abscess formation, chronic progression), and clinical manifestations (back pain, stiffness, and progressively developing neurological symptoms), the most likely diagnosis is tuberculous spondylitis (Pott's disease). If uncertainty remains, a lesion biopsy or specialized pathogen testing can be performed to confirm the diagnosis.
Treatment Plan and Rehabilitation Program
1. Medications and Conservative Treatment:
- Anti-tuberculosis therapy: According to relevant national and regional guidelines, combination anti-tuberculosis medications (typically 6–9 months or longer following standard protocols) are the first-line choice. Medication regimens should be adjusted by a physician based on drug sensitivity tests.
- Immobilization and bracing: For unstable vertebrae or pronounced kyphosis, a brace or external fixation can be used to reduce loading and facilitate vertebral healing.
- Symptomatic management: For significant pain, analgesics or anti-inflammatory medications may be used, while closely monitoring neurological function.
2. Surgical Intervention:
- If a large abscess is present, or if there is severe spinal cord compression, significant vertebral collapse, or spinal instability, surgical decompression, abscess debridement, and necessary internal stabilization may be considered.
- Postoperatively, continued systematic anti-tuberculosis therapy is necessary to prevent recurrence.
3. Rehabilitation and Exercise Prescription:
- Early stage: Prioritize protective training and safety; avoid excessive loading or large-amplitude trunk twisting. Low-intensity core stability exercises (e.g., modified planks, supine pelvic lifts) can be performed for 5–10 seconds each time, with adequate rest in between. Aim for 3–5 sets per day, progressively increasing the duration of each exercise.
- Intermediate stage: Once the condition is under control and inflammation is reduced, gradually introduce low-intensity aerobic exercises such as walking or using a stationary bicycle 3–4 times a week for 20–30 minutes each session, keeping the intensity at a level where one can maintain a normal conversation. Gentle stretching can be added to improve spinal muscle flexibility.
- Late stage: When the lesion is healing and spinal stability is achieved, gradually increase core strengthening exercises and back muscle resistance training. If necessary, introduce progressive weight-bearing exercises under professional guidance to promote spinal stability and functional recovery.
- Throughout the process: Adhere to the FITT-VP principle (Frequency, Intensity, Time, Type, and Progression), devise an individualized plan under the assessment of medical and rehabilitation professionals, and monitor for back pain or neurological abnormalities. If pain worsens or if there is numbness or weakness in the lower limbs, seek medical evaluation promptly.
Disclaimer: This report is for reference purposes only and does not replace a clinical consultation or professional medical diagnosis and treatment. If you have any questions or experience any discomfort, please consult healthcare professionals and seek in-person medical attention immediately.
Human Doctor Final Diagnosis
Tuberculous spondylitis (Pott's disease)