掌长肌的一种变异



临床病史
根据临床和影像学结果,确诊为掌长肌的附加远端肌腹。
影像学表现
该患者是一名体力劳动者,表现为右腕掌侧疼痛性肿胀。疼痛为间歇性,并在前臂肌肉剧烈使用时诱发。表面皮肤外观正常。
矢状面和轴向超声检查显示,在右桡侧腕屈肌腱内侧有一个界限清晰的肿物。该软组织肿块呈均质结构,与邻近肌肉回声相似。
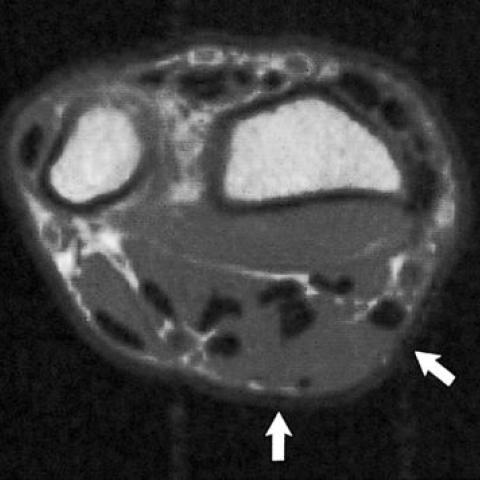
右前臂轴位SE T1加权MR图像显示,在桡侧腕屈肌腱内侧、屈肌支持带浅表处出现梭形肿物(箭头所示)。在T1及T2加权(未显示)图像上,该肿物与邻近肌肉信号均匀且等强度。
根据临床和影像学表现,诊断为掌长肌远端附加性肌腹。未进行手术或活检。
病情讨论
掌长肌是一条小型梭形肌,起自肱骨内侧髁。其远端部分为单一肌腱,附着于屈肌支持带浅层的掌腱膜。根据系统发育学,它被归类为退化性肌肉。
掌长肌是手部最具变异性的肌肉。缺如是最常见的变异,发生率为12.8%。肌腹可置于中部、呈二腹肌或分叉,或沿掌长肌整个走行延伸。起点和止点的变异或重复出现相对罕见。附加肌束是常见变异之一,可导致尺神经受压。当肌肉在屈肌支持带深面附着或在远端出现额外肌腹时,可能会引发伴有正中神经受压的腕管综合征。在过去50年的放射学文献中,掌长肌远端肌腹肥大的报道仅有三例。最近报道在42例正常手腕中有三例(7%)发现围绕掌长肌腱存在薄层肌纤维,但我们认为这三例可视为二腹型掌长肌,这种情况并不算罕见。
通过超声检查或MRI结合位置及信号特征可以对掌长肌变异进行诊断。临床症状及相关神经受压程度决定是否需要手术干预。
鉴别诊断列表
最终诊断
掌长肌
证书
(无内容)
图像分析
超声


右前臂轴向SE T1加权MR图像
医学影像分析报告
一、影像学发现
在超声和MRI图像中,可以观察到位于前臂远端、与桡侧腕屈肌及屈肌群邻近区域的异常肌肉组织。该肌腹与常规的掌长肌腱关系密切,且呈现出与周围肌群相似的信号强度。MRI横断面上可见一个位于前臂正中线附近的增厚肌肉带(箭头所示),与常见掌长肌腱的单纯腱形式不同,提示有额外或变异的肌腹存在。通过不同序列和切面的成像,未见明显骨质破坏或韧带结构异常。
二、潜在诊断
基于影像表现和患者的基本情况,可考虑以下诊断或鉴别诊断:
- 1. 掌长肌变异(副肌腹或附加肌腹):临床及影像学上常见的掌长肌缺失或变异,若肌腹增厚或位置异常,可导致局部肢体症状。
- 2. 腕部其他肌腱或肌肉变异:如屈指肌群或桡侧屈腕肌的变异,但通常位置与掌长肌腱不同,影像上可加以区分。
- 3. 腕关节囊性病变(如腱鞘囊肿):临床常见,超声下多表现为无回声或低回声,信号特征与肌肉组织不同,可与本例区分。
三、最终诊断
结合患者年轻男性的临床背景、影像所见肌肉信号及位置,与解剖变异的掌长肌副肌腹相吻合,最可能的诊断为:
“掌长肌远端附加肌腹(Accessory distal muscle belly of the palmaris longus)变异。”
若患者症状与该变异相关,则需要考虑进一步干预;若无明显临床症状,可定期随访。
四、治疗方案与康复计划
针对掌长肌远端附加肌腹的处理,可根据症状和神经受压情况进行个体化选择:
-
保守治疗:
若无明显腕管受压或临床不适,可先行观察和随访;配合物理治疗(热敷、局部肌肉牵伸、肌肉筋膜放松)及佩戴护腕以减轻局部肌腱或神经刺激。 -
手术治疗:
在出现明显神经受压、疼痛或功能障碍时,可考虑手术切除附加肌腹或行外科减压。术后需进行康复训练,恢复腕部的屈伸功能和抓握力量。
下述为简要的康复与运动处方范例(可根据患者耐受度与恢复进度灵活调整):
- 康复早期(术后或症状显著期):
- 频率:每周3~5天。
- 强度:轻度,避免明显疼痛或非正常不适。
- 时间:每次10~15分钟的温和拉伸与活动度练习。
- 方式:腕部关节主动屈伸、前臂旋前旋后,以及指关节主动活动。
- 进阶:在疼痛缓解并能完成日常活动后,逐渐增加轻度等长抗阻练习。
- 康复中期(症状减轻且已适应轻度运动):
- 频率:每周3~5天。
- 强度:中等强度,循序渐进使用弹力带或小哑铃。
- 时间:每次15~20分钟,结合腕部、前臂及手部的助力或抗阻训练。
- 方式:腕部屈伸抗阻练习、握力训练、手指关节灵活度练习。
- 进阶:待功能改善后可增加形式多样的协调性训练,如沙球挤握、柔软弹力球锻炼等。
- 康复后期(功能恢复期):
- 频率:每周3~5天。
- 强度:中等或稍高,密切监测疼痛与疲劳。
- 时间:每次20~30分钟,结合多种功能训练(可增加前臂力量、抓握力量的综合练习)。
- 方式:整体前臂主被动牵伸、抗阻训练,结合健身器械或功能性训练(如改良俯卧撑、引体向上辅助练习),注意动作规范。
- 进阶:根据上肢肌力与协调性,逐步回归运动或增强力量、灵活度的个人目标。
在上述康复过程中,应特别关注:若出现反复性疼痛、腕管区域麻木或不适加重,需及时与医疗团队联系并调整训练方案。
五、免责声明
本报告根据患者提供的病史与影像资料进行分析,仅供参考,不能替代面对面临床诊断与治疗。对于具体诊疗方案的确定,请向专业的骨科、手外科或康复科医生咨询。
人类医生最终诊断
掌长肌