Slipped upper femoral epiphysis



Clinical History
A 9-year-old boy with a history of prostatic embryonal rhabdomyosarcoma, treated with chemoradiotherapy and transurethral resection, presents with limping and hip pain on the left side. Lab results were normal. The boy was of normal weight and height. There was no recent trauma.
Imaging Findings
On the suspicion of transient synovitis of the hip, an ultrasound was performed. A unilateral joint effusion in the left hip was confirmed. However, when compared with the contralateral side, there was not only a joint effusion, but also an asymmetrical shape of the femoral head with a malalignment of 8 mm between the epiphysis and metaphysis. A pelvic MRI 9 months prior, showed no abnormalities in both hip joints.
After consultation with the paediatrics and orthopaedics department radiographic anteroposterior (AP) and frog-leg views of the pelvis were taken. Both views showed a clear slipped upper femoral epiphysis (SUFE). There also was a clear antalgic pelvic tilt to the left while performing the frog-leg position.
Discussion
Slipped upper femoral epiphysis (SUFE) is a type I Salter-Harris growth plate injury and is the most common hip disease of adolescence, with an incidence of 4.8/100000 in 0–16-year-olds [1]. SUFE occurs when repeated shearing forces applied on the femoral head exceed the strength of the capital femoral physis. Risk factors include: normal periosteal thinning and widening of the physis during rapid growth acceleration, trauma, obesity, inflammation, genetic predisposition, endocrine and metabolic disorders (hypothyroidism, hypopituitarism, hyperparathyroidism, renal osteodystrophy) and (as is the case in our patient) radiation and/or chemotherapy [2,3].
Plain radiographs are the most common imaging tool to evaluate SUFE. The minimal examination consists of an AP view and lateral projections of both hips. The lateral projections are most often obtained with a frog-leg view. When acute instability is suspected, alternatives like the cross-table lateral or true lateral pelvic view might be preferred to reduce the risk of further displacement. In the case of extreme obesity, other views like the unilateral Lauenstein view might be considered [4,5]. As the slip of the epiphysis is directed posterior and only to a lesser extent medial, lateral views are essential [6].
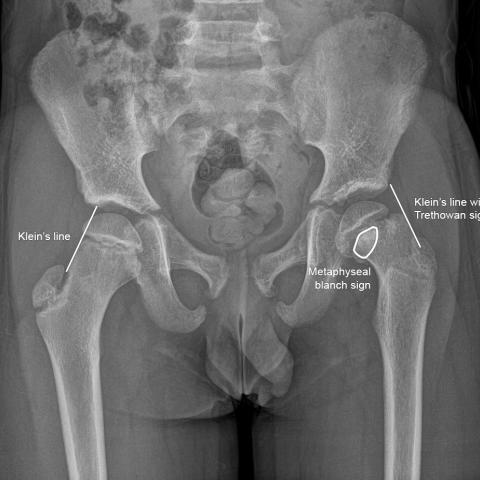
In the pre-slip stage, there is widening of the physis, with irregular and blurred edges of the metaphysis. Once the epiphysis has slipped posteriorly, it might appear smaller on AP views. The line drawn along the superior edge of the femoral neck (Klein’s line) on AP views fails to intersect the lateral portion of the femoral head as it passes outside of the epiphysis, known as the Trethowan sign. However, as this sign has a very low sensitivity, an overlap of 2 mm might be suggested as a threshold to increase sensitivity for SUFE [7]. Another sign of SUFE on AP views is the metaphyseal blanch sign, where superposition of the femoral neck and the posteriorly displaced capital epiphysis results in increased density [8]. On lateral views Southwick’s head-shaft angle is used to grade the severity of SUFE. A slip-angle of <30° is considered mild, 30-30° moderate and >60° is considered severe [8,9].
Ultrasound has little role in the routine evaluation of SUFE. Its use has been described in the diagnosis and follow-up of SUFE, and might even confirm the diagnosis when plain radiographs are normal. However, MRI is more commonly used as it can easily detect widening of the physis and surrounding oedema. Furthermore, MRI can assess the extent and distribution of osteonecrosis, if present [8].
All patient data have been completely anonymised throughout the entire manuscript and related files.
Differential Diagnosis List
Final Diagnosis
Slipped capital femoral epiphysis
Liscense
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Figures





I. Radiological Findings
Based on the provided pelvis anteroposterior (AP) and frog-leg lateral X-rays, the left femoral head epiphysis is observed to slip posteriorly and inferiorly relative to the femoral neck. On the AP view, the following characteristics are noted:
- The left femoral head epiphysis shows obvious displacement in relation to the femoral neck. Klein’s line (drawn along the superior lateral margin of the femoral neck) fails to intersect the lateral portion of the left femoral head, indicating a positive Trethowan sign.
- A “metaphyseal blanch” sign is visible.
- Compared to the contralateral side, the left physis (growth plate) region may appear widened.
Ultrasound imaging is limited but may occasionally provide hints of mild joint effusion or abnormal positioning of the slipped femoral head. Given the patient’s history and physical examination, ultrasound is not the primary diagnostic tool but can help assess the surrounding soft tissues.
II. Potential Diagnoses
Considering the patient’s age, symptoms, and previous history of tumor treatment, the primary possible diagnoses include:
- 1. Slipped Upper Femoral Epiphysis (SUFE):
This is a common hip disorder in children and adolescents, often occurring during rapid growth or in those with risk factors such as radiotherapy or metabolic disorders. Radiographically, it is characterized by posterior-inferior slippage of the femoral head epiphysis, with Klein’s line no longer intersecting the lateral portion of the femoral head, and the presence of the metaphyseal blanch sign, among other findings. - 2. Mild Avascular Necrosis (AVN) of the Femoral Head:
After chemotherapy and radiotherapy, compromised blood supply to the bone can occur. However, early AVN is often best detected by MRI, while X-rays typically show collapse or sclerosis only in later stages. - 3. Arthritis or Other Synovial Joint Disorders:
For example, transient synovitis or secondary synovitis following chemotherapy can cause hip pain. Laboratory tests (elevated inflammatory markers) or ultrasound may offer clues.
III. Final Diagnosis
Combining the above radiological findings, the patient’s age, previous history of chemo-radiotherapy, and current normal laboratory results, as well as normal height and weight, the most fitting diagnosis is:
Left Slipped Upper Femoral Epiphysis (SUFE).
For further evaluation, an MRI can be used to assess the physis and surrounding soft tissues, as well as to check for any compromise of the femoral head blood supply. However, based on conventional X-rays and clinical symptoms, SUFE is the most likely and appropriate diagnosis at present.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategies
- Conservative Treatment: For mild and stable slips, strict weight-bearing restrictions are required to prevent further slippage. Short-term bed rest or walking with crutches may be considered, with close monitoring.
- Surgical Fixation: Internal fixation with screws or pins is commonly performed to prevent further slippage, especially in marked or unstable slips. Surgery aims to stabilize the growth plate and prevent subsequent osteochondral injury or avascular necrosis of the femoral head.
- Follow-up Imaging: After fixation, regular X-ray or MRI follow-ups are necessary to observe physis healing and femoral head vasculature, so that any complications can be promptly identified and addressed.
2. Rehabilitation and Exercise Prescription Suggestions
Rehabilitation should be individualized and follow a progressive approach (FITT-VP: Frequency, Intensity, Time, Type, Progression, and Individualization). Because careful consideration of hip loading is crucial, the initial stage is best guided by a professional rehabilitation therapist.
- Early Stage (postoperative or early conservative treatment):
• Focus on limiting weight-bearing and gentle range-of-motion exercises. Non-weight-bearing or partial weight-bearing exercises, such as prone leg raises or light resistance band exercises, can be utilized.
• Frequency: 1–2 times per day, 10–15 minutes each time; Intensity: low, avoiding pain. - Intermediate Stage (pain relief, stabilized epiphysis):
• Increase range of motion and muscle strength around the hip and knee joints, such as seated or supine joint mobility exercises and small-range weight-bearing movements (like partial standing or short-distance walking with a walker or crutches).
• Frequency: 3–5 times per week; Intensity: moderate, with no significant pain. - Late Stage (functional recovery, transition to normal activities):
• Gradually restore bilateral lower limb strength, coordination, and stability through activities like seated cycling, swimming, or water walking to reduce impact on the hip.
• Frequency: 3–5 times per week; Intensity: moderate to slightly higher, progressing based on the patient’s recovery status.
During the entire rehabilitation process, the affected limb’s pain and range of motion should be closely monitored. If pain worsens or joint motion becomes restricted, re-evaluation and consultation with the physician are necessary. Because this patient has undergone chemo-radiotherapy, bone health and the recovery process may be more variable than in peers, requiring extra caution in rehabilitation.
Disclaimer
This report is a professional analysis based on existing imaging and clinical information for reference only. It cannot replace in-person consultation or professional medical advice. Specific treatment plans should be carried out under the guidance of a qualified specialist.
Human Doctor Final Diagnosis
Slipped capital femoral epiphysis