Plantar fasciitis


Clinical History
Heel pain.
Imaging Findings
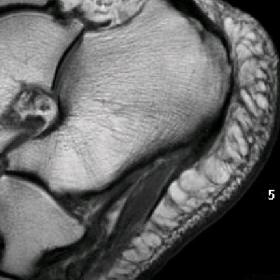
The patient presented with heel pain, which had increased in intensity over the previous few weeks and was especially severe in the morning. Sagittal T1-weighted MRI showed an increase in signal intensity and thickening in the proximal plantar fascia (Fig. 1). A sagittal T2-weighted FSE image showed oedema of the neighbouring soft tissues (Fig. 2). On a coronal STIR image bone marrow oedema centred on the origin of the plantar fascia was seen.
Discussion
Repetitive trauma and mechanical stress are the most frequent causes of plantar fasciitis. Microruptures and inflammatory changes of the fascia and perifascial tissues result. Plantar fasciitis is common in runners and obese people (1,2). Inflammations of the plantar fascia may cause heel pain even without preceding trauma (1). Pain is perceived at the origin of the fascia. It is enhanced by dorsiflexion of the toes and it is more severe in the morning.
The lateral radiograph often shows a spur. This finding is unspecific however, because it is found in 25% of the symptom-free population. Scintigraphy may show increased uptake in the calcaneal region indicating a periostal inflammation (1). MR imaging is able to differentiate plantar fasciitis from other causes of heel pain, e.g. ruptures of the plantar fascia (1,2). On sagittal or coronal MR images the physiological plantar fascia is a thin, signal-free bandlike structure that extends anteriorly from the ventral undersurface of the tuber calcanei. The normal thickness of the plantar fascia is 3.22mm +/- 0.44mm and it flares at its calcaneal origin. Inflammatory changes result in thickening of the fascia and a signal increase in all sequences (intermediate signal on PD and T1-weighted images, high signal on T2-weighted images), These changes are pronounced in the proximal part of the fascia. Oedema may be seen in the subcutaneous fat and deep tissues, as well as bone marrow oedema centred on the origin of the fascia. The thickening of the fascia is often fusiform, which differs from plantar fibromatosis with its more focal, nodular thickening. In cases of rupture discontinuity of the fascia, oedema and haemorrhage can be seen.
Therapy is initially conservative, including orthesis and administration of non-steroidal antirheumatics. In more severe cases local injection of steroids and even resection of the fascia may be necessary.
Differential Diagnosis List
Final Diagnosis
Plantar fasciitis
Liscense
Figures
Sagittal T1-weighted MRI

Sagittal T2-weighted FSE image

Coronal STIR image

Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided MRI images, marked thickening of the plantar fascia (primarily at its origin along the medial calcaneal border) is observed. On T1-weighted sequences, the fascial signal is mildly increased, and on PD or T2-weighted sequences, a hyperintense signal can be seen, suggesting local edema and inflammation. The fascia thickening appears fusiform, especially near the calcaneal attachment, with mild surrounding soft tissue edema. No significant fascial discontinuity is noted, and there is no clear evidence of a large-scale tear. A mild abnormal signal in the adjacent calcaneal bone marrow may indicate bone marrow edema or inflammatory changes.
II. Potential Diagnoses
- Plantar Fasciitis: The most common clinical and imaging manifestation is thickening of the proximal fascia with hyperintense signal changes, often accompanied by local edema. It frequently occurs in individuals who stand, walk, or run for prolonged periods, as well as those with obesity.
- Plantar Fibromatosis: Typically presents as a more localized nodular or mass-like thickening, usually without significant surrounding edema. The T2-weighted signal may be relatively heterogeneous. If a focal nodular lesion is observed on the images, consider this diagnosis.
- Partial or Complete Tear of the Plantar Fascia: Characterized by disruption of fascial continuity with significant surrounding edema and hemorrhagic-like signal. If the patient reports acute, tear-like pain or has a history of trauma, a fascial tear should be ruled out.
III. Most Likely Final Diagnosis
The patient is a 62-year-old female presenting with hindfoot pain, which aligns with the common presentation of plantar fasciitis. Imaging findings demonstrating significant thickening of the plantar fascia near the calcaneal attachment, altered signal, and possible calcaneal bone marrow edema strongly support a diagnosis of plantar fasciitis.
IV. Treatment Plan and Rehabilitation Program
- Conservative Treatment:
- Rest and Reduced Weight-Bearing: Limit prolonged standing and walking, and avoid high-impact activities such as running or jumping.
- Orthotic Devices or Arch Support Insoles: Use arch supports to reduce tension on the plantar fascia.
- NSAIDs: Short-term use to alleviate inflammation and pain.
- Local Physical Therapy: Ice application, ultrasound, or other modalities to help reduce inflammation.
- Indications for Injection and Surgery:
- Local Steroid Injection: May be considered under physician guidance if conservative treatments are insufficient.
- Surgical Treatment: In very rare, severe, or refractory cases, partial fascial release may be considered when all other measures fail or in cases of severe recurrence.
- Rehabilitation/Exercise Prescription:
- Gradual Progression Under the FITT-VP Principle:
- Frequency: 3–5 times per week for stretching and strengthening.
- Intensity: Stretch to a moderate tension without significant pain; use bodyweight or resistance bands for strengthening.
- Time: 10–20 minutes per session, performed in sets (e.g., 3–5 sets of stretching, holding each stretch for 20–30 seconds).
- Type: Plantar fascia stretching (using a towel or wall for support), calf stretching, and strengthening exercises for the foot and ankle (e.g., toe towel grabs or small heel raises).
- Progression: As pain subsides and function improves, gradually increase the intensity and duration of stretches or introduce balance exercises.
- Special Precautions:
- If the patient has osteoporosis or other chronic systemic conditions, exercises should be performed under the guidance of a physician or rehabilitation specialist.
- Discontinue activities and seek re-evaluation if significant pain or any other discomfort arises during exercise.
- Gradual Progression Under the FITT-VP Principle:
Disclaimer
This report is based on the available images and clinical information, providing general reference recommendations only. It does not replace an in-person diagnosis or an individualized treatment plan by a professional physician. If you have any concerns or if symptoms worsen, please seek further evaluation at a hospital without delay.
Human Doctor Final Diagnosis
Plantar fasciitis