Acro-osteolysis in hyperparathyroidism


Clinical History
Increased tiredness and pain in the hands.
Imaging Findings
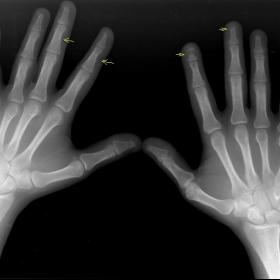
The patient complained of increased tiredness and pain in his hands. Blood tests and radiographs of his hands were performed. The blood tests revealed hypercalcaemia. Radiographs of the hand showed erosions of the tufts (tips) of the terminal phalanges and sub-periosteal erosions along the radial aspect of the middle phalanges. Also noted was resorption of the middle portion of a few of the phalanges. As part of the work-up, further radiographs of the knee joints were performed, which showed sub-periosteal erosion along the superio-medial aspect of the tibiae. A hyperfunctioning parathyroid adenoma was also noted, for which surgery was performed.
Discussion
In acro-osteolysis there is loss of terminal tufts of the digits. No periosteal reaction is seen. Epiphyses, if involved, occur late in the disease. It is seen is various conditions including:
- Scleroderma (associated with soft calcifications)
- Psoriatic arthritis, associated with nail and skin deformities
- Hyperparathyroidism, other findings include sub-periosteal resorption along the radial side of the middle phalanges
- Cleidocranial dysostosis
- Pyknodysostosis, along with aplasia/hypoplasia of the distal digits and seen in children
- Polyvinylchloride exposure, workers with history of exposure
- Progeria, premature ageing
- Hajdu-Cheney Syndrome (familial idiopathic acro-osteolysis), rare syndrome and may be unilateral
- Frostbite
- Neuropathic, secondary to diabetes, syringomyelia etc
The patient in this case, in addition to hypercalcaemia, had other changes of hyperparathyroidism secondary to a parathyroid adenoma: sub-periosteal resorption seen at the proximal tibia bilaterally (Fig. 2) and along the radial aspect of the middle phalanges and resorption of the middle portion of the phalanges.
Differential Diagnosis List
Final Diagnosis
Acro-osteolysis in hyperparathyroidism
Liscense
Figures
AP view of both hands with coned view of the distal phalanges


AP view of both knee joints

1. Radiological Findings
From the bilateral hand X-ray in the frontal view, the following can be observed:
- Partial bone resorption of the distal phalanges (digital tuft), presenting as osteolysis of the terminal phalanx (also referred to as "acro-osteolysis").
- Evidence of subperiosteal bone resorption, especially on the radial side of the middle phalanges of the fingers and near the proximal tibia (this may also be visible on the bilateral tibia X-rays in different projections).
- Consistent with clinical reports, the patient has hypercalcemia, indicating a possible metabolic abnormality.
The frontal radiograph of both tibiae shows similar localized subperiosteal bone resorption along the medial or proximal shaft region, further corroborating a systemic bone metabolism disorder.
2. Potential Diagnoses
Based on the patient’s history (male, 40 years old, recent fatigue, hand pain, and hypercalcemia) and the radiographic findings (acro-osteolysis and subperiosteal resorption), the following differential diagnoses should be considered:
- Scleroderma: May present with acro-osteolysis but is often accompanied by skin thickening and vascular manifestations (e.g., Raynaud’s phenomenon).
- Psoriatic arthritis: Distal phalangeal destruction is frequently associated with skin changes and nail abnormalities such as pitting or psoriasis lesions.
- Secondary causes related to specific exposures or rare genetic disorders (e.g., polyvinyl chloride exposure, Hajdu-Cheney syndrome): Radiographic findings may also show distal phalangeal resorption; occupational or family history is essential for further evaluation.
- Hyperparathyroidism: Characteristically shows subperiosteal resorption (especially along the radial aspects of the phalanges) in conjunction with hypercalcemia; chronic disease can lead to diffuse bone changes and skeletal pain.
Considering the combination of elevated serum calcium, subperiosteal resorption, and acro-osteolysis, hyperparathyroidism is the most representative potential diagnosis.
3. Final Diagnosis
Taking into account the patient’s age, clinical symptoms (fatigue, hand pain), laboratory data (hypercalcemia), and X-ray findings (acro-osteolysis and subperiosteal bone resorption), the most likely diagnosis is:
Primary Hyperparathyroidism (suspected to be caused by a parathyroid adenoma)
Confirmation typically requires further blood tests (e.g., parathyroid hormone [PTH] levels) and neck imaging (e.g., ultrasound, CT, or nuclear medicine scan) to assess the parathyroid glands.
4. Treatment Plan and Rehabilitation Program
4.1 Treatment Strategy
- Surgical Treatment: For primary hyperparathyroidism due to a parathyroid adenoma, surgical removal of the adenoma is often performed to control excessive PTH secretion and hypercalcemia.
- Pharmacological Therapy: If surgery is not currently feasible, consideration can be given to using bisphosphonates (e.g., clodronate, zoledronic acid) to reduce bone resorption, or employing calcimimetic agents (e.g., cinacalcet) to help control serum calcium levels.
- Management of Comorbidities: Monitor bone density, renal function, and other metabolic abnormalities. Supplement with vitamin D as needed.
- Diet and Lifestyle: Regulate calcium intake (according to an individualized plan by the physician) and regularly check electrolytes.
4.2 Rehabilitation and Exercise Prescription
For patients with bone metabolism disorders but without severe osteoporosis or high risk of fracture, a gradual, low-impact exercise regimen may be recommended, following the FITT-VP principles:
- Frequency: 3–5 times per week, adjusted appropriately under professional guidance depending on fatigue.
- Intensity: Begin with low to moderate intensity such as walking, jogging, or cycling, ensuring adequate warm-up and avoiding sudden heavy loads.
- Time: Approximately 20–40 minutes each session, adjusted based on individual tolerance and medical advice.
- Type: Low-impact aerobic exercises (e.g., swimming, elliptical training) combined with gentle resistance training (using resistance bands or light weights).
- Progression: Gradually increase exercise duration or intensity within tolerable limits, typically adjusting every 2–4 weeks. Avoid excessive increases that may cause fatigue or injury.
- Volume & Pattern: Split sessions are acceptable (e.g., one 30-minute session or three 10-minute sessions). Incorporate muscle strength training to support bone health.
If the patient exhibits significant osteoporosis or severe bone pain, follow individualized training supervised by specialist physicians and rehabilitation therapists to minimize fall and fracture risks.
Disclaimer
This report is based solely on the available imaging and clinical history and is intended for reference only. It does not replace an in-person consultation or professional medical advice. The definitive diagnosis and treatment plan should be made by the attending medical team after comprehensive clinical evaluations and further testing.
Human Doctor Final Diagnosis
Acro-osteolysis in hyperparathyroidism