Hand-Schuller-Christian disease



Clinical History
The patient presented with local pain, swelling , tenderness of the thigh, and loose teeth. There were not any systemic signs or symptoms.
Imaging Findings
The patient presented with local pain, swelling , tenderness of the thigh, and loose teeth. There were not any systemic signs or symptoms.
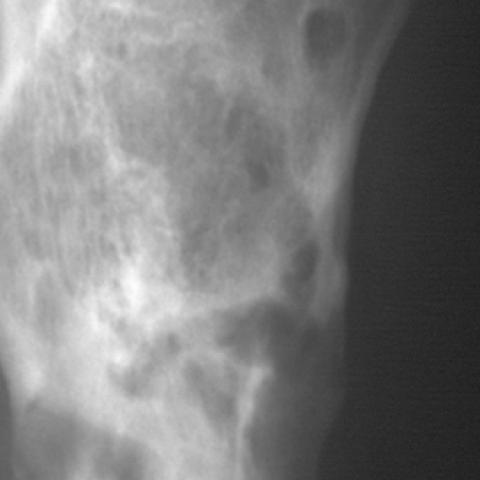
Plain radiographs of the skull showed large lesions, giving the appearance of "geographic skull" and "floating teeth". Radiographs of the femur and pelvis showed multiple lytic lesions with ill-defined borders, including one lesion of the acetabulum.
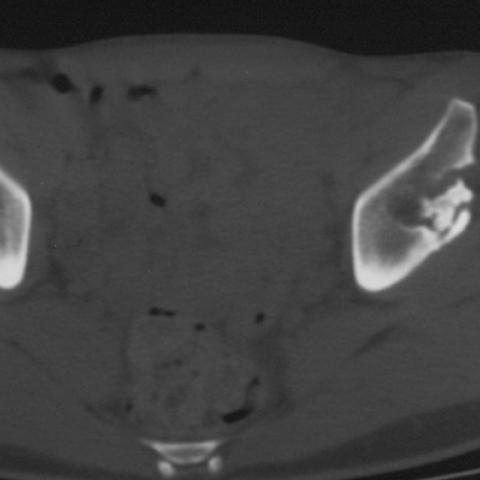
Computer tomography of the pelvis and femur showed lytic leasions with disruption of the cortex and small soft tissue mass.
MRI of the hips and femur showed isotense lesions on T1-weighted images, which showed enhacement with gadolinium, and high signal areas of bone replacement on T2-weighted images.
Discussion
Hand-Schuller-Christian disease is a chronic disseminated form of histiocytosis X, in which idiopathic non-neoplastic proliferation of histiocytes occurs. It may involve any bone, but preferred sites are the skull, mandible, spine and long bones. The lesions may be well defined or poorly defined with or without associated sclerotic borders. A variable amount of periosteal reaction can be present, ranging from a thick solid type to lamellated.
In the skull, lesions usually have sharply defined borders with uneven involvement of the inner and outer table. At the centre of the lytic process a button sequestrum may appear. Large lesions give the appearance of "geographic skull". In the mandible and maxilla, bone destruction may produce the appearance of "floating teeth".
In the spine, typically, there is lysis of affected vertebrae leading to progressive collapse (vertebra plana) with preservation of adjacent disc space, which usually allows distinction from infection.
In the long bones, lesions usually arise in the diaphysis or metaphysis and are centred in the medullary cavity causing endosteal scalloping and eventually cortical penetration. The lesions may also appear as permeative lesions with ill-defined borders and periosteal reaction. Bone scintigraphy is of limited usefulness. CT may be useful to define the extent of the process. On MRI examination, T1-weighted images reveal a lesion isointense to adjacent tissue and T2-weighted images reveal high signal areas of marrow replacement.
The differential diagnosis includes:
- Skull lesions: osteomyelitis, epidermoid cyst.
- Long bones (aggressive form): round cell lesions, Ewing's sarcoma, osteosarcoma, leukaemia, acute osteomyelitis.
- Long bones (less aggressive form): simple cysts, fibrous dysplasia, chronic osteomyelitis.
- Vertebra plana: leukaemia, metastatic neuroblastoma, idiopathic osteonecrosis.
Differential Diagnosis List
Final Diagnosis
Hand-Schuller-Christian disease
Liscense
Figures
Plain radiographs


Computed tomography images



Magnetic resonance imaging



Medical Imaging Analysis Report
I. Radiological Findings
Based on the provided imaging data (CT/MRI of the skull, maxillofacial region, femur, and pelvis), the main observations are as follows:
- Skull and Maxillofacial Region:
- On skull X-ray, scattered “punched-out” lytic lesions can be seen in the cranial bones, with relatively clear or slightly unclear boundaries. In some areas, a “geographic skull” appearance is observed.
- Obvious bone destruction is noted in the jawbones, with some affected teeth showing a “floating teeth” sign, indicating significant alveolar bone resorption.
- Femur and Pelvis:
- In the proximal segment or metaphysis of the femur (as seen on X-ray or CT/MRI), there are lytic lesions. In some areas, the internal margins are destroyed; mild cortical bulging or irregular periosteal reaction may be present.
- Pelvic CT shows a lytic lesion in the iliac bone with unclear boundaries and reduced bone density in the region. On MRI T1-weighted images, the lesion signal is comparable to or slightly lower than the adjacent bone marrow, whereas on T2-weighted images it appears hyperintense, suggesting replacement or infiltration of the bone marrow.
- Clinical Correlation:
- The patient reports loose teeth, and together with the “floating teeth” sign in the jaw, there is a high suspicion of localized bone destruction involving the alveolar bone.
- Local pain and tenderness in the thigh correspond to the site of the lesion; soft tissue swelling or effusion may be present, but there are no obvious systemic symptoms.
II. Potential Diagnoses
Considering the patient’s age (23 years old), clinical presentation (loose teeth, thigh swelling and pain), radiological findings (skull “punched-out” lesions, “floating teeth” sign, lytic changes), and references from the literature, possible diagnoses include:
- Langerhans Cell Histiocytosis (including Hand-Schüller-Christian disease and other subtypes)
Commonly presents with lytic lesions involving the skull, jaw, long bones, and vertebrae, and may feature the floating teeth sign and geographic skull changes. It is relatively common in younger patients. - Infectious Bone Disease (e.g., Chronic Osteomyelitis)
Lytic destruction and periosteal reactions may be seen, but usually accompanied by significant inflammatory signs such as fever, local redness, and elevated white blood cell counts. This case does not present clear evidence of systemic infection. - Malignant Bone Tumors or Tumor-like Lesions (e.g., Ewing’s Sarcoma, Metastatic Bone Lesions, Leukemic Bone Involvement, etc.)
Certain small round cell tumors or hematologic malignancies can present with lytic destruction, but they often accompany systemic symptoms or other abnormal laboratory findings. The patient in this case does not have evident systemic symptoms or reported abnormalities in blood tests. - Other Cystic Bone Lesions (such as Simple Bone Cysts or Fibrous Dysplasia)
They often present with clearer boundaries and may or may not have sclerotic rims. However, the floating teeth sign in the jaw and multiple lytic lesions are not typical in these conditions.
III. Most Likely Final Diagnosis
Integrating the patient’s age, local symptoms (femoral pain and swelling, loose teeth), the multifocal bone lysis observed on imaging (skull, jaw, femur, and pelvis), as well as the characteristic “floating teeth” sign and “geographic skull” changes, the most likely diagnosis is Langerhans Cell Histiocytosis (Hand-Schüller-Christian type).
Further confirmation may involve a pathological biopsy (demonstrating proliferation of Langerhans cells, Birbeck granules, etc.) and relevant immunohistochemical staining (CD1a, S100 protein positivity). Endocrine evaluation (to exclude or confirm pituitary involvement) and whole-body nuclear medicine scans can also be performed to assess the extent of disease.
IV. Treatment Plan and Rehabilitation
1. Treatment Strategy
- Pharmacotherapy: For single or limited bone lesions, local steroid injections may be considered. Widespread disease requires systemic glucocorticoid therapy, chemotherapy, or immunomodulators.
- Surgical/Interventional Therapy: For extensive local lesions causing structural destruction or functional impairment, procedures such as curettage and bone grafting can be considered; in some cases, low-dose radiotherapy may also be an option.
- Supportive Care: Maintain adequate nutritional status, ensure oral hygiene management (loose teeth may require extraction or periodontal support), and pay attention to bone health.
2. Rehabilitation/Exercise Prescription
The rehabilitation and exercise prescriptions should be tailored to the patient’s lesion distribution, bone strength, and overall health status, following a gradual and individualized approach:
- Initial Stage:
- Focus on low-intensity lower-limb functional training, avoiding high-impact or heavy-load activities (e.g., running, jumping) to reduce the risk of fracture.
- Consider non-weight-bearing or low-weight-bearing exercises, such as seated or partial weight-bearing leg extensions, stationary cycling, or aquatic rehabilitation.
- Frequency: 3–4 times per week; each session about 20–30 minutes, starting with low intensity.
- Intermediate Stage (after the condition stabilizes):
- Gradually increase the intensity of weight-bearing exercises, such as using resistance bands for lower-limb strengthening, and incorporate overall coordination and flexibility training.
- Frequency: 4–5 times per week; each session 30–40 minutes, with a subjective feeling of slight exertion (RPE scale about 11–13).
- Later Stage (after bone healing or disease remission):
- Depending on bone healing and pain status, gradually resume light running, gentle jumping, and other impact exercises, while monitoring for pain or swelling.
- Frequency: 4–5 times per week; session length can be increased to 40–60 minutes. Consider adding core muscle and balance training to help prevent re-injury.
- Individual Adjustments:
- If there is increased local pain, signs of fracture, or noticeable discomfort during training, stop immediately and seek medical attention.
- Regular follow-up of bone density, imaging studies, and laboratory tests is recommended. Coordination with medical specialists and rehabilitation therapists is essential to adjust the exercise types and intensity in a timely manner.
FITT-VP Principle: Frequency, Intensity, Time, Type, Progression, and Individualization should be planned comprehensively according to the patient’s current condition, bone status, safety, and tolerance.
Disclaimer: This report provides a reference-based analysis and does not replace in-person consultation or professional medical advice. Specific diagnostic and therapeutic plans should be determined according to the patient’s actual situation and evaluated by a qualified medical professional.
Human Doctor Final Diagnosis
Hand-Schuller-Christian disease