


Complaints of mild local pain in the right distal forearm.
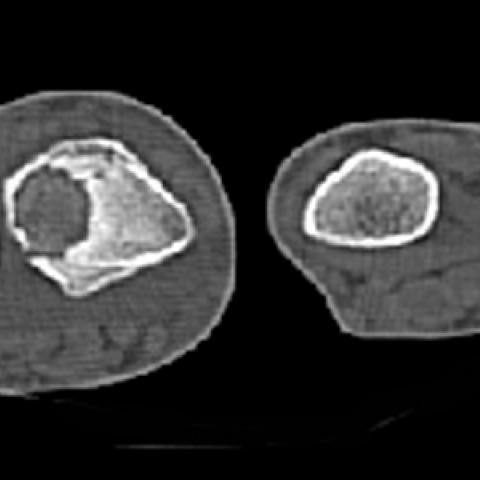
The boy presented with mild local pain in the right distal forearm. X-ray film showed a large oval radiolucent expansile lesion, surrounded by a zone of bone sclerosis, in the metaphysis of the radius with cortical thickening. A reactive periosteal reaction in the ulna was also seen. CT revealed disruption of the radius cortex with surrounding soft tissue edema or infiltration. 3D volume rendering CT reconstruction clearly showed the lesion in the radius, surrounded by bone sclerosis.
Osteoblastoma is a richly vascular tumour characterised by an abundance of osteoblasts. Although the histopathology is similar to osteoid osteoma, clinically and radiographically the two lesions differ [1]. Male patients are affected more frequently than female patients, in a ratio of 2:1, and 75% of patients are between 10 and 30 years of age, with a peak incidence in the second decade. The spine is the preferred site (37%), and most osteoblastomas localise in the arch of the vertebrae (pedicle, lamina, and spinous process) and sacrum [2]. A smaller number have a predilection for the shafts of long bones (upper extremity 7%, lower extremity 25%). An important feature that distinguishes osteoid osteoma from osteoblastoma is the size of the lesion. Osteoid osteoma is a small tumour, rarely exceeding 1 cm and is self-limiting. Osteoblastoma, however, is a large lesion (average 3.5 cm); it is rarely under 2 cm and may enlarge to 10 cm.
As in cases of osteoid osteoma, local pain is a common manifestation of osteoblastoma [3], although generally it is mild. Accentuation of pain at night and its amelioration with salicylates are inconstant clinical features of osteoblastoma. Spinal lesions may be accompanied by muscle spasm, scoliosis, and neurological manifestations, including paresthesias and weakness.
The radiographic features of osteoblastoma are varied and differ from the singular expression of an osteoid osteoma. It simulates one of the following three basic roentgenologic patterns: an osteoid osteoma, an aneurysmal bone cyst or a malignant bone tumor [4]. Whereas osteoblastoma resembles an osteoid osteoma, the nidus is consistently larger than 2 cm. If the tumor arises eccentrically in a bone and involves the cortex, sclerosis can be prominent. In the long tubular bones, osteoblastomas may originate in the medullary or cortical bone or, rarely, in a subperiosteal location. Variable in size and sometimes quite large, these lesions usually are round or oval and predominantly osteolytic, with areas of calcification or ossification, well marginated, and expansile. Bone sclerosis and periostitis may be exuberant, and the latter finding may resemble the periosteal reaction that characterizes malignant neoplasms. In the spine, a well-defined, expansile osteolytic lesion that is partially or extensively calcified or ossified, arising from the posterior osseous elements, especially in the thoracic or lumbar segment, should suggest the diagnosis of an osteoblastoma [4]. Osteoblastomas are infrequent in the skull. The precise location is variable. They present as a circumscribed oval radiolucent defect, with varying degrees of central calcification, involving both the inner and the outer tables of the skull. Bone scintigraphy, CT scanning, and MR imaging can be used to assess osteoblastomas. Bone scintigraphy reveals increased accumulation of the radionuclide at the site of the lesion, and CT scanning and MR imaging allow full delineation of the extent of the process. An inflammatory reaction in the bone affected by the tumor or in the nearby soft tissues may lead to a misleading appearance in MR images that simulates a malignant tumor. This inflammatory reaction may include a mass that reveals enhancement of signal intensity following the intravenous administration of a gadolinium compound. There are no focal lesions visible on the T1-weighted image, but edema is present. The T2-weighted image shows edema in the marrow as well as the surrounding soft tissues. Differentiation between malignant and benign appearances can be difficult with MR [5].
Osteoblastoma





1. The X-ray images show a relatively localized and clearly eccentric lesion in the right distal forearm radius (near the diaphyseal-metaphyseal region), with a certain degree of bony expansion.
2. On CT images, there is significant bony destruction and a low-density area within the lesion; the local boundary is relatively clear. Part of the lesion contains high-density or calcified signals, suggesting bony or calcified components.
3. Surrounding bone displays a certain degree of reactive sclerosis and cortical thickening; patchy or punctate ossification can be seen in some areas.
4. The internal structure of the lesion shows mixed density with a relatively clear margin and an expansile growth pattern. No clear evidence of soft tissue mass protrusion is noted.
5. No obvious involvement of the articular surface is seen, and there is no significant swelling or extensive abnormal signal in the surrounding soft tissues.
Based on the patient’s age (15 years), clinical presentation (mild local pain), and imaging findings (>2 cm expansile lesion, internal calcification/ossification, local sclerotic reaction), the following diagnoses are considered:
Taking into account the patient’s age, lesion size (clearly exceeding 2 cm), imaging characteristics (expansile bone destruction with partial ossification, a relatively clear sclerotic rim), and only mild pain, the most likely diagnosis is Osteoblastoma.
If any diagnostic uncertainty remains or if confirmation of benign versus malignant nature is required, a biopsy of the lesion can be performed for histopathological examination.
1. Treatment Strategy:
- Surgical Treatment: For a confirmed osteoblastoma, curettage or curettage plus bone grafting is typically the first-line treatment. Extended local resection may be necessary depending on the lesion. If the resection is extensive, postoperative internal fixation and bone reconstruction should be considered to ensure stability and prevent fracture.
- Medications and Symptomatic Management: Short-term use of NSAIDs can help relieve pain depending on the patient’s symptom severity.
- Postoperative Follow-up: Regular imaging follow-up is needed to monitor for tumor recurrence and assess bone healing.
2. Rehabilitation Exercises and Exercise Prescription (FITT-VP Model):
- Early Postoperative Phase (Acute Phase):
· Emphasis on protecting the surgical region and avoiding excessive weight-bearing.
· Non-weight-bearing or immobilized isometric muscle contractions can be performed to maintain muscle tone and promote local circulation.
· Frequency: 1–2 times a day; Intensity: Light; Time: 5–10 minutes each session; Type: Mainly static muscle exercises in a safe position; Progression: Gradually increase the number of sessions and duration according to pain level and wound healing.
- Mid-Postoperative Phase (Recovery Phase):
· Once bone healing is stable, a gradual transition to partial weight-bearing exercises can be introduced, such as assisted lower-limb or contralateral upper-limb exercises, to promote bone and soft-tissue recovery.
· Frequency: 3–4 times per week; Intensity: Light to moderate; Time: 15–20 minutes each session; Type: May include low-resistance exercises (small weights/bands) and range-of-motion exercises; Progression: Gradually increase resistance or difficulty.
- Late Phase (Functional Reconstruction Phase):
· After confirmation of a stable lesion and clear bone healing, higher-intensity forearm muscle and joint functional training can be carried out, such as grip-strength exercises, joint flexibility drills, and multi-directional wrist and forearm rotation exercises.
· Frequency: 3–5 times per week; Intensity: Moderate; Time: 20–30 minutes each session; Type: May integrate strength training, stability training, and light aerobic activities (e.g., stationary cycling, swimming); Progression: Gradually increase intensity and load as long as there is no significant pain or discomfort.
- Notes:
· Close observation of pain, swelling, or other discomfort during training is essential. If unusual symptoms occur, seek medical attention or consult a rehabilitation therapist promptly.
· Progressively increase exercise volume according to the patient’s bone health and cardiopulmonary capacity, avoiding excessive fatigue and re-injury.
Disclaimer: This report is based solely on the available imaging and medical history. It does not replace an in-person evaluation nor the professional opinion of a physician. Actual diagnosis and treatment should be determined by a professional medical team, in combination with the patient’s specific condition.
Osteoblastoma