Lipoma arborescens



Clinical History
A 30-year-old woman presented with a history of chronic pain and an intermittent swelling of both her knees. A physical examination revealed bilateral swelling in the suprapatellar region. An MR examination of the left knee was performed.
Imaging Findings
The MR images demonstrated a synovial thickening in the suprapatellar bursa, with a signal intensity similar to that of fat on all pulse sequences, without joint effusion. After a gadolinium injection was administered, foci of synovial enhancement could be seen on the MRI.
Discussion
Lipoma arborescens is a rare benign synovial disease characterized by villous lipomatous proliferation. The knee is the most commonly involved joint, with a predilection for the suprapatellar pouch. Bilateral involvement may occur. The clinical presentation includes a slow increase in swelling of the joint, usually over many years, associated with intermittent joint effusion. The erythrocyte sedimentation rate is found to be normal and the joint fluid aspirate is found to be sterile. Two patterns can be seen on MR images: a diffuse lipomatous thickening of the synovium, or the presence of synovial mass-like fat deposits. Joint effusion is often associated, while bone erosions are an infrequent occurrence. The differential diagnosis includes pigmented villonodular synovitis, which is characterized on an MR examination by the low signal intensity of hemosiderin deposition on T2-weighted images. Synovial osteochondromatosis and chronic rheumatoid arthritis are responsible for a low to intermediate signal on T1-weighted images. A synovial lipoma presents as a solitary round mass of fat without synovial changes. A synovial hemangioma contains foci of low signal intensity corresponding to the enlarged vessels of phleboliths. The treatment of choice for this condition is a synovectomy.
Differential Diagnosis List
Final Diagnosis
Lipoma arborescens.
Liscense
Figures
Figure 7

Figure 6
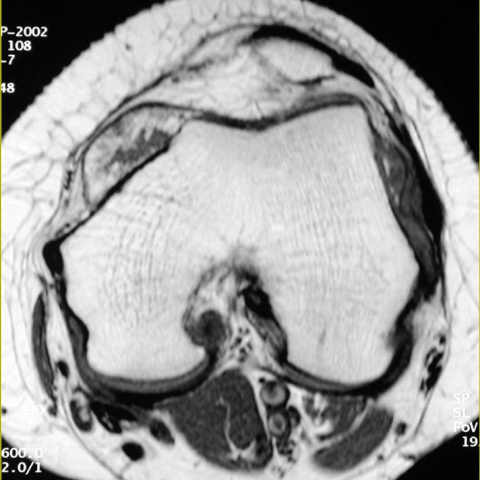
Figure 5

Figure 4

Figure 3

Figure 1

1. Imaging Findings
Based on the MRI images of the patient’s knees, bilateral knee joints (with onset mainly in the left knee) show abnormal soft tissue thickening in the synovial regions, primarily in the suprapatellar pouch (suprapatellar bursa). This proliferative tissue demonstrates high signal on both T1- and T2-weighted images, similar to the signal of adipose tissue. There are signs of joint effusion, but no evident bone erosion or bony destruction. Overall, the synovium appears villous or arborized, indicating a “fatty” pattern.
2. Potential Diagnoses
Taking into account the patient’s chronic knee pain, recurrent joint swelling, and MRI findings, possible imaging differential diagnoses include:
- Lipoma Arborescens: Proliferation of adipose tissue within the joint synovium, usually appearing as high signal on T1- and T2-weighted images, often accompanied by joint effusion. This correlates with the patient’s clinical history of long-term recurrent swelling and normal inflammatory markers (e.g., normal ESR).
- Pigmented Villonodular Synovitis (PVNS): Typically shows low signal on T2-weighted images due to hemosiderin deposition; may present as hypertrophic or nodular synovium, but this case lacks the typical T2 low-signal nodules.
- Synovial Osteochondromatosis: Often features intra-articular or peri-synovial loose bodies or cartilaginous nodules, usually with low to intermediate T1 signal and potential calcifications, none of which are evident in this case.
- Synovial Lipoma: Characteristically an isolated lipomatous lesion without pronounced diffuse synovial proliferation, and not necessarily linked to chronic joint effusions.
- Synovial Hemangioma: Can present with localized low signal on MRI (due to vessels, thrombi, or calcification), but no typical hemangioma features are noted in this case.
3. Final Diagnosis
Considering the patient’s age, clinical presentation, normal lab results (e.g., normal ESR, sterile joint fluid), and the MRI findings of “fatty” synovial thickening, the most likely diagnosis is:
Lipoma Arborescens.
Further confirmation usually does not require a biopsy. However, if clinical suspicion remains, arthroscopic evaluation and synovial biopsy can be performed to exclude other rare conditions.
4. Treatment Plan and Rehabilitation
4.1 Treatment Strategy
- Arthroscopic or Surgical Synovectomy: For patients with significant symptoms or notably impaired joint function, arthroscopic or surgical synovectomy can effectively alleviate symptoms, reduce joint effusion, and lessen the likelihood of recurrence.
- Conservative Management: If symptoms are mild, initial treatment may involve joint immobilization, short-term use of non-steroidal anti-inflammatory drugs (NSAIDs) for pain and inflammation control, along with close observation of disease progression.
- Follow-up: Include regular imaging and clinical assessments to watch for changes in joint effusion or synovial thickness, as well as to monitor for relapse.
4.2 Rehabilitation and Exercise Prescription
During both post-surgical and conservative management phases, to reduce knee pain, prevent muscle atrophy, and facilitate early functional recovery, a step-by-step rehabilitation plan following the FITT-VP principle can be employed:
- F (Frequency): Start at 1–2 sessions per week, gradually increasing to 3–4 sessions per week as the joint adapts.
- I (Intensity): Focus on low to moderate intensity exercises, avoiding activities with high impact (such as deep squats, running, or jumping) to protect the knees.
- T (Time): Begin with 15–20 minutes per session, gradually extending to about 30 minutes. Intermittent training may help avoid prolonged weight-bearing.
-
T (Type):
- Seated or supine passive range-of-motion exercises to restore joint flexibility.
- Straight leg raises, quadriceps strengthening drills, and other low-intensity movements for muscle conditioning.
- Moderate joint activities (e.g., stationary cycling, swimming/hydrotherapy) to reduce impact on the knee.
- V (Volume): Combine session duration and frequency to progressively increase total training volume, while closely monitoring joint tolerance.
- P (Progression): As pain subsides and range of motion/muscle strength improves, gradually increase load by incorporating foam rolling, resistance bands, and other functional exercises. Transition slowly to moderate resistance training (e.g., light squats or seated leg presses), ensuring no significant pain arises.
Throughout rehabilitation, avoid sudden increases in activity level and closely monitor for recurring joint swelling or exacerbated pain. If symptoms recur significantly, prompt review and adjustment of the rehabilitation plan is advised.
Disclaimer: This report is based on the analysis of existing images and clinical information for reference purposes only. It cannot replace in-person consultation or professional medical advice. If you experience any discomfort or special circumstances, please seek medical attention promptly.
Human Doctor Final Diagnosis
Lipoma arborescens.