Extra-nodal recurrence of follicular B-cell lymphoma



Clinical History
A 81 years old woman referring a slightly growing mass in the left arm since 4 months.
Imaging Findings
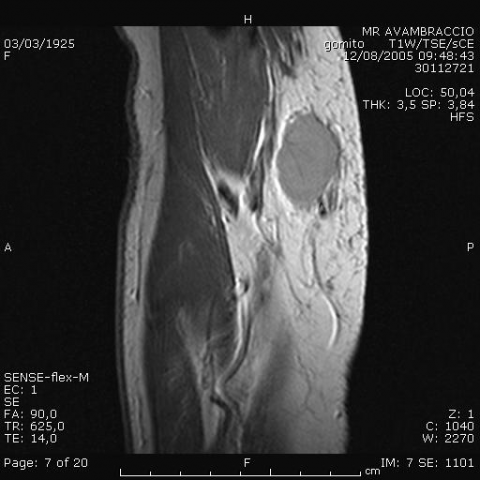
A 81 years old woman was treated for non-Hodgking B-cell lymphoma of the abdomen in 1983. The patient's history revealed in 1995 a right gluteal recurrence with complete remission after treatment with radiotherapy. She referred in 1997 a surgical ablation of a not precisely defined shwannoma in the lateral left arm. Now she presented for an enlarging painless soft-tissue mass in the medial proximal left arm. Ultrasonography revealed a 2.8 cm well-defined hypoechoic solid mass, showing apparently a pseudocapsule and anarchic vascolarization at Color-Doppler. MR imaging confirmed the presence of a fusiform solid mass in the bicipital region of the proximal left arm, isointense on T1 weighted images and hyperintense on T2 STIR images with the normal muscle, with fairly homogeneous diffuse enhancement after paramagnetic contrast administration.
Discussion
Although lymphomas are neoplasm of lymph nodes, the involvement of other tissues can occour (20-30%). The subcutaneous tissue can rarely be affected and the lymphomatous nodules can be either solitary or multiple and can be a prymary presentation or a subsequent recurrence. At sonography lymphomatous nodule is hypoechoic with a psudocapsule and sometimes fibro-adiopse septa inside. The usefulness of CT in evaluation of extra-nodal subcutaneous lymphoma is not specific, showing an enlarging hypodense mass with slight enhancement after contrast. MR imaging is superior to other tecniques for its soft-tissue contrast and multiplanar imaging capability. Lymphomas are relatively homogeneous on MR, only 6% has non-homogeneous pattern that can be attributed to its intrinsic heterogeneity. On average, lymphomas were hypointense to fat and slightly hyperintense to muscle in T1-weighted images but isointense to fat and hyperintense to muscle in T2-weighted images, with slight enhancement after contrast media. Low-, intermediate-, and high-grade non-Hodgkin lymphomas had identical imaging characteristics. Usually Hodgking lymphomas are brighter for their fibrosis in T2-weighted than non-Hodgkin lymphomas.
Differential Diagnosis List
Final Diagnosis
Recurrent follicular B-cell lymphoma in adipose tissue of left arm
Liscense
Figures
Ultrasonography

MR imaging- axial TSE T1w

MR imaging- sagittal TSE T1w

MR imaging- axial TSE T2w

MR imaging- sagittal TSE T2w with fat suppression

MR imaging- sagittal TSE T1 w after contrast media e.v.
Ultrasonography with color-Doppler

Radiological Findings
Based on ultrasound and magnetic resonance imaging (MRI) images, the mass is located in the subcutaneous tissue of the left upper arm. It appears as a round or oval-shaped hypoechoic nodule with relatively well-defined boundaries. Ultrasound shows that the lesion is hypoechoic internally, with a visible pseudo-capsule sign around it, and it may have fibrous fatty septa inside. MRI demonstrates that on T1-weighted images, the lesion signal is slightly lower than fat and slightly higher than or similar to surrounding muscle, while on T2-weighted images, the lesion signal is relatively homogeneous and high. Mild to moderate enhancement can be observed after contrast administration.
The lesion measures approximately 2–3 cm in diameter (according to imaging), with clear margins and no obvious signs of infiltration into the surrounding soft tissue. No significant bone destruction or cortical abnormality is noted. Adjacent structures (such as muscles and fascia) remain relatively intact.
Potential Diagnoses
- Subcutaneous Lymphoma: Lymphoma can primarily or secondarily involve subcutaneous tissue, typically presenting as a relatively homogeneous soft tissue mass on imaging, with increased T2-weighted signal and absent or minimal enhancement, matching the characteristics in this case.
- Subcutaneous Soft Tissue Sarcoma (e.g., Liposarcoma or Fibrosarcoma): Soft tissue sarcomas may also present as subcutaneous masses. However, their MRI often shows more marked heterogeneity, necrosis, or cystic changes, and their margins may be less clearly defined compared to lymphoma.
- Metastatic Lesion: Subcutaneous metastases commonly occur with malignant melanoma or other solid tumors. Given that there is no documented history of other malignancies (based on current information), this possibility is relatively lower in this case.
- Inflammatory Lesion or Granuloma: If the patient has a history of local trauma, injection, or infection, one should consider granuloma or abscess; however, imaging typically would show more pronounced inflammatory signs and fluid components.
Final Diagnosis
Considering the patient's advanced age (81 years), presentation as a slow-growing subcutaneous solid mass, the homogeneous hypoechoic features on ultrasound and high T2 signal on MRI, and the mild enhancement after contrast, the most likely diagnosis is subcutaneous lymphoma. If subtype differentiation (Hodgkin's or Non-Hodgkin's) is necessary, a histological biopsy (fine-needle or surgical) and further immunohistochemistry and pathology are recommended for confirmation and treatment guidance.
Treatment Plan and Rehabilitation
Once confirmed pathologically as lymphoma, treatment options typically include:
- Chemotherapy: For Non-Hodgkin's or Hodgkin's lymphoma, standard chemotherapy regimens (e.g., CHOP or ABVD) may be used. Specific drugs and cycles depend on pathology subtype and staging.
- Radiotherapy: If the lesion is localized and not large, local radiotherapy may be considered as part of adjuvant or curative treatment.
- Immunotherapy or Targeted Therapy: For instance, the anti-CD20 monoclonal antibody rituximab can be used in the treatment of Non-Hodgkin's lymphoma.
- Surgical Management: If the mass affects local function or requires a definitive diagnosis, biopsy or partial resection can be performed. However, surgery alone is generally not the first choice for curative treatment of lymphoma.
Concerning rehabilitation and exercise, it is recommended to implement a gradual exercise program based on the patient's physical condition and tolerance of adjuvant therapies (chemotherapy/radiotherapy) to maintain and improve muscle strength, physical fitness, and quality of life:
- Frequency (F): 3–5 times per week, adjusted according to the patient's tolerance.
- Intensity (I): Begin with low intensity (such as seated leg raises, shoulder shrugs) and progressively move toward moderate intensity (such as slow walking, gentle cycling). Monitor heart rate, blood pressure, and subjective fatigue to ensure safety.
- Time (T): Initial sessions of 10–15 minutes, increasing gradually to 20–30 minutes as tolerance improves.
- Type (T): Emphasize safe, low-impact aerobic activity and light resistance training, such as easy walking, seated cycling, or using resistance bands.
- Progression (P): Gradually increase session duration or mildly increase resistance, ensuring safety. If the patient experiences fatigue or discomfort, pause or reduce exercise intensity.
- Special Considerations: Due to the patient's advanced age and potential chemotherapy, precautions against falls, fractures, and infections are essential. Professional guidance by a rehabilitation therapist or trainer is recommended.
During subsequent rehabilitation, regular follow-up of the disease course and physical function assessment is warranted. Adjust the exercise plan as needed. Additionally, monitoring for chemotherapy and radiotherapy side effects—such as bone marrow suppression, fatigue, and skin or mucosal damage—is crucial, and prompt communication with the clinical physician is advised.
Disclaimer
This report is based on the current imaging findings and clinical data, provided for reference only and not a substitute for an in-person consultation or professional medical advice. If you have any questions or new symptoms arise, please seek medical attention promptly. For a definitive diagnosis and treatment plan, further examinations under the guidance of a clinical physician are necessary.
Human Doctor Final Diagnosis
Recurrent follicular B-cell lymphoma in adipose tissue of left arm