Tibial Tuberosity Avulsion Fracture in Puberty -Surgical Management-Rare Images



Clinical History
A case report of a 14-year-old boy who has sustained sports injury (Salter Harris injury type III) to his left upper tibia. This case is published in terms of rarity at puberty, type of surgical fixation and the imageries, has never been reported in the literature.
Imaging Findings
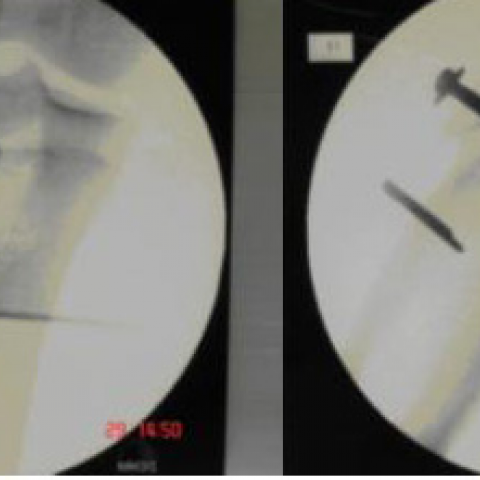
A fit 14-year-old young boy whilst doing high jump, felt a sudden sharp pain and swelling in his knee joint. He was unable to weight bear. Examination showed a spindle shaped swelling of his left knee. Generalized tenderness and a high riding patella were noted. All movements of knee joint were severely restricted by pain. X-rays (Fig1) showed a tibial tuberosity avulsion fracture with tibial epiphysis involvement. Under General anesthetic, the fragments were reduced (Fig.2) and fixed with a 50 mm cancellous screw and a staple (Fig.3). He was given a plaster cast for two weeks till suture removal. He was then fitted with a non-weight bearing knee brace for four weeks allowing full knee movements. Then he was allowed to weight bear fully. He has been rehabilitated with physiotherapy. His wound and fracture healing is good. He has now returned to all activities.
Discussion
Discussion: Review of literature showed only 76 fractures reported since 1935. Only 33 were type III. Type III fractures were most often observed in older adolescents from 15-17 years of age, whereas types I & II fractures were most often noted in adolescents from 12-14 years of age. According to Shelton and Canale,3 the frequency of tibial tubercle avulsion treated at a large medical centre is only once in every 4 years, with type III being even more rare. The rarity of separation can be explained by its circumferential reinforcement by capsule and soft tissues of knee joint.4 Donald et al published a case report of 15 years old boy who sustained injury to his right knee while playing basket ball had type III avulsion fracture. After three and half months later, he sustained avulsion fracture on the other side as well1. There is a common consensus, that open reduction & internal fixation is the treatment of choice in type I& III avulsion fracture. Suture, staples, metallic pins or screws are used for fixation. Blount warned of the possibility of Genu Recurvatum deformity in theory in young adolescent after a type III fracture. Nonetheless, so far epiphyseal arrest was not reported in any patient. Levi and Coleman7 acknowledged excessive compression by internal fixation across an epiphyseal plate will lead to adverse effects. We are reporting type III fracture in a pubertal age group, which is very rare. No reports of growth disturbance of the proximal tibial epiphysis occurring after a type III fracture have been found.1
Differential Diagnosis List
Final Diagnosis
TIBIAL TUBEROSITY TYPE III FRACTURE IN PUBERTY- IMAGES PUBLISHED
Liscense
Figures
Pre-Op X Rays

Per Operative picture

Post- Op C-ARM Images
1. Imaging Findings
Based on the provided X-ray and intraoperative fluoroscopic images, a fracture line is visible in the proximal left tibia (primarily involving the tibial tuberosity region). The fracture fragment is clearly separated from the main tibial body, consistent with the typical features of a Salter-Harris Type III (physis) fracture. The fracture fragment mostly involves or is adjacent to the articular surface, with some mild displacement seen. Intraoperative images show a clear avulsion of the tibial tuberosity and soft tissue stripping, necessitating internal fixation to restore anatomical alignment and joint stability. No large-scale tear of the surrounding soft tissues (ligaments, tendons) is evident on imaging, and the joint space appears acceptable; however, potential hidden soft tissue damage should be considered.
2. Potential Diagnoses
- Salter-Harris Type III physeal separation (tibial tuberosity avulsion fracture)
Reason: The patient is in adolescence with ongoing skeletal development. Imaging shows a fracture at the proximal tibial physis extending to the articular surface. The typical avulsion fracture site is at the tibial tuberosity. - Tibial plateau fracture (upper tibial segment)
Reason: If the fracture line extends into the articular surface with displacement, a tibial plateau fracture should be considered. However, given the patient’s age and the physis involvement, a Salter-Harris injury is more likely. - Acute exacerbation or severe avulsion in Osgood-Schlatter disease
Reason: Osgood-Schlatter disease is a common overuse condition in adolescents, affecting the tibial tuberosity. However, imaging typically shows chronic ossification center prominence rather than a clearly visible acute fracture line.
3. Final Diagnosis
Combining the patient’s age of 14, history of sports-related injury, and findings on X-ray and intraoperative observation, the diagnosis is: Salter-Harris Type III physeal separation (avulsion fracture) of the left tibial tuberosity. This case is relatively rare, especially in mid-adolescence. No other obvious fractures or severe soft tissue injuries are observed. If further assessment of articular cartilage or ligament damage is needed, MRI should be considered for more precise evaluation.
4. Treatment Plan & Rehabilitation Program
Treatment Strategy:
- Surgical Treatment: For Salter-Harris Type III fractures, open reduction and internal fixation (e.g. screws or metal pins) is typically used to ensure proper alignment of the fracture and a smooth articular surface, reducing the risk of long-term joint dysfunction and physeal damage.
- Postoperative Protection: After surgery, bracing or casting may be applied as needed to protect the fixation and limit excessive flexion-extension movements.
Rehabilitation/Exercise Prescription (FITT-VP Principle):
- Phase 1 (0-2 weeks postoperative):
• Frequency: Perform 2-3 sessions per day of gentle joint activity exercises (e.g. ankle pumps, isometric quadriceps contractions).
• Intensity: Low intensity, avoiding direct weight bearing on the surgical area.
• Time: About 5-10 minutes per session.
• Type: Primarily bedside quadriceps exercises and non-weight-bearing joint mobilization; if no specific contraindications, passive knee flexion and extension exercises can be done in sitting or supine position.
• Progression: Gradually increase range of motion as wound healing progresses and pain subsides. - Phase 2 (2-6 weeks postoperative):
• Frequency: 3-5 rehabilitation or physical therapy sessions per week.
• Intensity: Gradually increase to light-moderate. Start partial weight-bearing with crutches support.
• Time: 15-20 minutes each session, including both range-of-motion and muscle-strengthening exercises.
• Type: Introduce static or low-resistance exercises (e.g. straight leg raises, light resistance bands) and knee flexion-extension within a tolerable range.
• Progression: Increase walking duration and joint range of motion as pain and swelling improve. - Phase 3 (6-12 weeks postoperative):
• Frequency: 3-5 times per week, adjusted according to recovery status.
• Intensity: Moderate intensity, gradually introducing full weight-bearing activities.
• Time: 20-30 minutes per session, including muscle strengthening and proprioceptive training.
• Type: Focus on joint stability (e.g. balance boards, closed-chain exercises such as partial squats) and low-impact aerobic exercises (stationary cycling, swimming, etc.).
• Progression: Transition to more functional exercises as muscle strength and joint stability improve. - Phase 4 (3-6 months postoperative and beyond):
• Frequency & Intensity: Progressively return to high-intensity weight-bearing or specialized sports activities, based on individual needs.
• Type: Incorporate running, jumping, and directional change drills, keeping an eye on pain and swelling during exercise.
• Safety: Discontinue or reduce load and seek evaluation if discomfort arises.
Special Notes: Follow-up X-rays or other imaging should be performed regularly to evaluate fracture healing and physeal status. As adolescents are still growing, early closure of the physis or deformity should be monitored. If abnormalities are detected, timely intervention is essential.
Prognosis: If reduction and fixation are accurate, most patients have a good functional recovery. Excessive or inappropriate local pressure should be avoided to prevent physeal damage or delayed joint instability.
Disclaimer: This report content is based solely on the provided clinical and imaging information for analysis and is intended only as a reference for medical decision-making. It does not substitute an in-person evaluation or professional medical advice. Specific diagnosis and treatment should be determined by a professional medical team considering the patient’s actual condition.
Human Doctor Final Diagnosis
TIBIAL TUBEROSITY TYPE III FRACTURE IN PUBERTY- IMAGES PUBLISHED