Achilles tendon abscess with focal osteomyelitis of calcaneum



Clinical History
A 76 year old diabetic male patient was referred to the vascular surgeons for a chronic right foot ulcer which was refractory to treatment. An initial x-ray revealed no obvious abnormality. Further imaging was done with MRI which revealed achilles tendon abscess with focal osteomyelitis of the calcaneum.
Imaging Findings
A 76 year old diabetic male patient was referred by his general practitioner to the vascular surgeons and orthopaedicians for a chronic right foot ulcer which was refractory to treatment. On clinical examination, there was a 3 cm ulcer in the heel of the right foot. There was some sensory loss in the heel of the foot and the pedal pulses were not palpable. X-ray of the right foot did not show any gross abnormality. A MRI was done which showed that the ulceration was directly over the posterior calcaneum. There was a small 1cm area of abnormal signal change noted within the marrow of the calcaneus postero laterally. This was of low signal on T1 images and high signal on T2 and fat suppressed images. Following gadolinium there was enhancement of this region consistent with inflammatory change or focal osteomyelitis. Also the lateral half of the achilles tendon inferiorly at the site of ulceration showed gross destruction. On T1 images there was diffuse intermediate signal replacing much of the tendon with only some normal low signal fibres being seen medially. On T2 images this area was of high signal. There was rim enhancement of the periphery of the achilles tendon following gadolinium. The tendon was expanded and appearances were suggestive of a large abscess in the achilles tendon. Surgical debridement was carried out and appropriate antiniotics were administered which resulted in good clinical improvement.
Discussion
Most of the pedal infections occur in patients with foot ulcers that result from predisposing conditions such as diabetes, vascular disease or neuropathy. Diabetic patients are predisposed to foot infections because of a compromised vascular supply secondary to diabetes. Local trauma and/or pressure (often in association with lack of sensation because of neuropathy), in addition to microvascular disease, may result in a variety of diabetic foot infections. The spectrum of foot infections in diabetes ranges from simple superficial cellulitis to chronic osteomyelitis. Skin ulceration occurs in areas of highest pressure during ambulation and most frequently involves the plantar aspect of the metatarsophalangeal joints, especially the first and fifth rays, the first toe, and the heel. Tendons in these locations are often situated over a bony prominence where ulceration occurs and are covered only by skin and a thin layer of subcutaneous tissue. As the infection of the soft tissues progresses, bacteria may invade and a long-standing, chronic infection may eventually lead to the destruction of the tendon. In the setting of soft tissue infection, it is extremely important to find out if there is any infection of the adjacent bone and tendons as this will affect the management. Plain x-rays are the most commonly performed initial investigation. However, it cannot pick up the early cases of osteomyelitis and result in considerable delay in diagnosis. Radio-nuclide studies are more sensitive but less specific. Also neither of these studies will be able to reveal the extent of tendinous involvement. In this regard, MRI is most useful for the diagnosis of tendon infection and osteomyelitis. Circular peritendinous contrast enhancement in the setting of a tendon in direct contact with adjacent skin ulceration or cellulitis is highly suggestive of tendon infection. In the case of Achilles tendon, as there is no tendon sheath, purists call it paratendinitis rather than tenosynovitis. Focal isointense or hypointense signal compared with muscle tissue on T1-weighted images with fluid equivalent signal on T2-weighted images and rim enhancement on gadolinium-enhanced T1-weighted images are suggestive of abscess. If there was osteomyeltis, it will be seen as an area of focally decreased marrow signal intensity on T1-weighted images with increased signal intensity on fat-suppressed T2-weighted and fast spin-echo short tau inversion recovery images and with marrow enhancement on gadolinium-enhanced fat-suppressed T1-weighted images. Treatment involves appropriate antibiotics with surgical debridement.
Differential Diagnosis List
Final Diagnosis
Achilles tendon abscess with focal osteomyelitis of calcaneum
Liscense
Figures
MRI of right foot

STIR image

T1 weighted image

T1 image showing the achilles tendon abscess
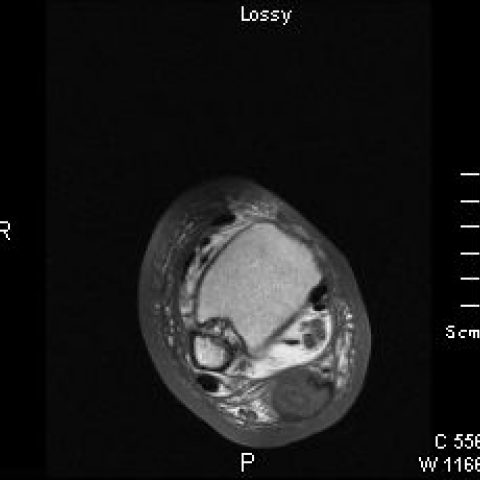
Post contrast scan

Medical Imaging Analysis Report
1. Imaging Findings
Based on the provided MRI images, the following observations can be made:
- Achilles tendon region: There is local soft tissue swelling, and significant abnormal signals around the Achilles tendon. On T1-weighted images, it appears iso- or low-signal, and on T2-weighted images, there is prominent high-signal intensity. Post-contrast images show ring-shaped enhancement at the edges, suggesting a local abscess or infectious lesion.
- Calcaneus: Localized bone marrow signal changes are noted. On T1-weighted images, it appears as low signal; on T2-weighted images and STIR sequences, it shows high signal. After contrast, bone marrow enhancement is observed, which is consistent with focal osteomyelitis.
- Surrounding soft tissues: Diffuse edema signals are apparent, especially near the Achilles tendon and calcaneus, which aligns with chronic inflammation or infection.
In summary, the MRI suggests abscess formation in the right Achilles tendon area and focal osteomyelitis of the calcaneus, consistent with infection-related findings.
2. Possible Diagnoses
- Achilles tendon abscess with tendon infection: Given that the Achilles tendon is close to the subcutaneous tissue, chronic ulcers can easily lead to deep infections. MRI findings of ring enhancement and fluid signals are consistent with an abscess.
- Calcaneal osteomyelitis: Patients with diabetes have poor blood supply, which predisposes to bone infection. Imaging shows low signal on T1, high signal on T2, and enhancement after contrast, typical features of osteomyelitis.
- Other soft tissue infections or chronic foot ulcers complicated by deep tissue infection: Differential diagnoses may include foot soft tissue inflammation, cellulitis, or peritendinitis. However, imaging and clinical presentations are more suggestive of Achilles tendon abscess and osteomyelitis.
3. Final Diagnosis
Considering the patient’s advanced age, history of diabetes, chronic foot ulcers, MRI findings, and characteristic lesion changes, the most likely diagnoses are:
- Achilles tendon abscess/infection (“paratendinitis” or soft tissue abscess)
- Localized osteomyelitis of the calcaneus
If further etiological clarification is needed, puncture or surgical exploration with pathological and microbiological culture can be performed to identify the causative organism.
4. Treatment Plan and Rehabilitation
-
Pharmacotherapy:
- Use antibiotics based on microbiological results or empirical therapy targeting Gram-positive bacteria (such as Staphylococcus aureus) and common Gram-negative bacteria. The course of treatment is usually prolonged (several weeks to months).
- Actively control blood glucose and maintain stable levels to facilitate wound healing; adjust antidiabetic medications or insulin dosage as needed.
-
Surgical Intervention:
- For abscess formation or necrotic bone areas, surgical debridement is required to remove necrotic and infected tissue, reducing the microbial load.
- If necessary, partial Achilles tendon repair or bone graft surgery may be performed; however, adequate evaluation of blood supply, soft tissue conditions, and infection control is essential prior to surgery.
-
Rehabilitation and Exercise Prescription:
- Early stage: Emphasize immobilization or weight-bearing reduction to prevent further damage to the Achilles tendon or spreading of infection. Use assistive devices or crutches for partial weight-bearing ambulation.
- Intermediate stage: Once the infection is stabilized, gradually resume mild ankle and foot movements, including active and passive ankle range-of-motion exercises. Each session can last 10-15 minutes, 2-3 times a day. Monitor for recurring pain or swelling in the affected area.
- Later stage: After complete healing of the surgical or debrided area and resolution of local pain and inflammation, progressively increase strength training (e.g., foot plantarflexion and dorsiflexion with resistance bands) and extend walking time or distance. Increase exercise frequency based on individual tolerance, aiming for 3-5 sessions per week, 20-30 minutes each session.
- Individual adjustments: Patients with diabetes and peripheral neuropathy should pay special attention to foot sensation and skin integrity. Inspect feet before and after exercise to detect any new ulcers or blisters promptly.
FITT-VP Principle Recommendations: Frequency gradually progresses from 2-3 sessions per week to 3-5 sessions; Intensity starts from very light or light exercise, monitoring foot response; Time increases from 10-15 minutes per session; Type includes walking and resistance band or ankle stability training; Progression is based on healing status and subjective tolerance, with moderate increases every 2-4 weeks.
5. Disclaimer
This report is based on the provided imaging and clinical information, serving as a reference analysis only. It does not replace an in-person consultation or professional medical advice. Should there be any questions or worsening of symptoms, the patient is advised to seek prompt medical attention for further examination and treatment by a qualified specialist.
Human Doctor Final Diagnosis
Achilles tendon abscess with focal osteomyelitis of calcaneum