Loose bodies in the knee: a common case with unusual presentation



Clinical History
We present a case of multiple loose bodies in the knee joint of a mentally retarded diabetic patient.
Imaging Findings
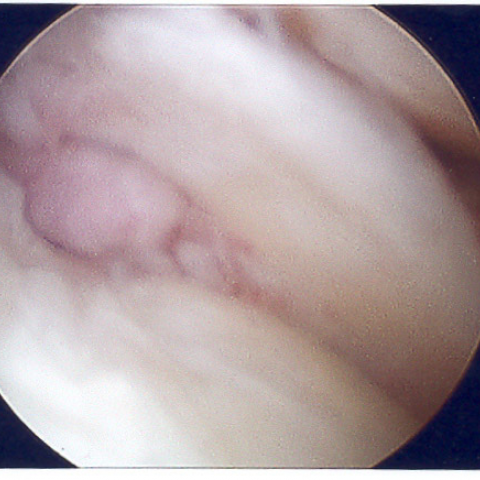
A 39-year-old mentally retarded lady was referred by the GP to the Orthopaedic Clinic with complaints of crepitations during movement of left knee. The attendant also mentioned that she had locking and giving away of the left knee. On examination, the left knee was normal in appearance with some swelling but there was no feature of inflammation. There was crepitation on movement. Drawer's tests were negative; varus and valgus tests were also negative. A plain x-ray of both knees AP and Lateral views were done that showed presence of multiple radio-opaque shadows in the left knee with mild osteoarthritic changes in the tibiofemoral and patellofemoral joints. A few loose bodies were also noted in the suprapatellar bursa. However, the right knee was alright both clinically and radiologically. The orthopaedic Surgeon decided to do knee arthroscopy. During the procedure, a total of 32 loose bodies were removed. They were all of the size of approximately 1cm in diameter with the largest one of about 2.5 cm in diameter. There was a mild arthritic change in the femoral surface. However, the articular surface was intact and there was no feature of osteochondritis dissecans. After the procedure, patient became asymptomatic and was discharged from the clinic.
Discussion
Loose bodies in the knee are not uncommon in Orthopaedic practice1, 3, 4. They develop for a variety of reasons. The commonest source of loose bodies in the knee is osteochondritis dissecans where there is osteocartilagenous separation of the articular surface at the subchondral level7. Other less common causes are osteophytes, torn meniscus, synovial osteochondromatosis8 and fractured bone. They can also be calcified, fibrous, bony, cartilaginous and osteocartilaginous in nature. The loose bodies range in size from very small3 to large particles, the former being called ‘snow storm knee’ for their appearance during arthroscopy4, 8. The loose bodies can be found anywhere in joint cavity including lateral recess of knee2. This is diagnosed on the basis of clinical findings and plain x-ray. Ultrasound can be done to detect the location and size of the loose bodies6. Our patient was mentally retarded and was under care of a carer. She was not able to communicate with others well and so it was suspected that the patient might have the loose bodies in the knee for a long time. The carer noticed the difficulty only lately. However, as there was no clear history of traumatic injury to knee, presence of multiple loose bodies only in left knee while other knee is normal can exclude traumatic cause. During arthroscopy, some osteoarthritic features were noticed in the femoral articular surface. But there was no feature suggestive of osteochondritis dessicans. So, the cause is highly likely to be synovial osteochondromatosis that have formed by encapsulation of niduses in layers for a long time5.
Differential Diagnosis List
Final Diagnosis
Multiple loose bodies in the knee
Liscense
Figures
X-ray of left knee


Loose bodies in the knee


Medical Imaging Analysis Report
I. Imaging Findings
Based on the provided X-ray images of both knees in the anteroposterior and lateral views, multiple round or nearly round dense shadows can be seen in the left knee joint. These are distributed within the joint cavity, including the suprapatellar bursa and the synovial regions around the joint. The shapes and sizes vary, with some displaying higher density, consistent with free bodies that have undergone calcification or ossification. The right knee appears normal, with no similar lesions observed. The continuity of the articular surface bone is generally intact, but mild changes on the distal femoral articular surface of the left knee indicate the presence of mild degenerative changes. No obvious narrowing of the joint space is noted. According to intraoperative findings, multiple scattered masses were removed; macroscopically, they appear spherical or nearly spherical, vary in size, and some show layered structures.
II. Potential Diagnoses
- 1. Synovial Osteochondromatosis
Multiple intra-articular loose bodies, especially a large number of calcified or ossified bodies, commonly arise from synovial proliferation forming multiple osteochondral nodules. These nodules are covered by synovium and accumulate in the joint space, matching the imaging characteristics and clinical presentation in this case. - 2. Osteochondritis Dissecans
Often involves detachment of bone-cartilage fragments from the articular weight-bearing surface, forming loose bodies. Typically, the number of loose bodies is smaller, and an obvious bone-cartilage defect is usually noted on the articular surface. While there are mild degenerative changes in this case, no typical osteochondral detachment or defect is seen, and the number of loose bodies far exceeds what is typical for osteochondritis dissecans. - 3. Degenerative Joint Disease with Loose Bodies
Advanced knee osteoarthritis can produce intra-articular loose bodies (e.g., detached osteophytes), but these are usually smaller in size and fewer in number. The high number of loose bodies in this case is not typical of simple degenerative joint disease.
III. Final Diagnosis
Taking into account the clinical history (intellectual disability, diabetes, and delayed detection due to communication difficulties), the imaging findings (numerous dense intra-articular shadows of varying sizes), arthroscopic confirmation of multiple bony or cartilaginous loose bodies, and the observed layered encasement upon cross-section, the most likely and fitting diagnosis is:
Synovial Osteochondromatosis.
If further confirmation is needed, pathological examination may be considered. Typically, it would reveal proliferative synovium with the formation of cartilaginous or bony tissue.
IV. Treatment Plan and Rehabilitation Program
1. Treatment Strategies
- Surgical Treatment: Arthroscopic debridement is the main approach, allowing removal of intra-articular loose bodies and partial synovectomy to prevent further proliferation. If there is evident cartilage damage or joint degeneration, cartilage repair or other reconstructive procedures can be considered.
- Conservative Treatment: If clinical symptoms are mild, and the number of loose bodies is small or the surgical risk is significant, observation, joint mobility guidance, and joint support (e.g., bracing) may be considered. However, given the large number of loose bodies and functional impairment in this case, arthroscopic debridement is still recommended.
- Medication: There is no specific pharmacotherapy, but nonsteroidal anti-inflammatory drugs (NSAIDs) can be used for symptomatic relief of pain and inflammation. In cases of poorly controlled blood sugar, better glycemic management should be ensured to promote healing.
2. Rehabilitation/Exercise Prescription Suggestions (FITT-VP Principle)
Postoperative rehabilitation should focus on restoring joint range of motion, muscle strength, and gradually resuming weight-bearing activities. The progression can be guided as follows:
- Frequency (F): 3-5 times per week, gradually increasing according to recovery.
- Intensity (I): Begin with low-resistance or isometric exercises to avoid excessive joint loading. Progress to gentle resistance exercises (e.g., resistance bands, light weights) in the later stages.
- Time (T): Each session of 20-30 minutes, possibly split into multiple shorter sessions to prevent fatigue.
- Type (T):
- Joint mobilization exercises and passive range-of-motion exercises
- Seated or semi-reclined leg raises (isometric and isotonic quadriceps training)
- In the later stages, incorporate low-impact aerobic activities such as stationary cycling or swimming
- Progression (P): Increase training load and range of motion as the knee joint function improves. Balance training under the guidance of a physical therapist may be introduced if necessary.
Special Considerations: For patients with diabetes, closely monitor blood glucose levels to prevent postoperative wound-healing complications. In addition, pay attention to safe weight-bearing and daily activities.
Disclaimer: The above report is a reference medical analysis based on currently available information and does not replace an in-person consultation or professional medical advice. Specific treatment plans should be determined in accordance with clinical findings and in consultation with qualified healthcare professionals.
Human Doctor Final Diagnosis
Multiple loose bodies in the knee